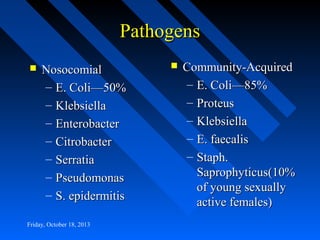
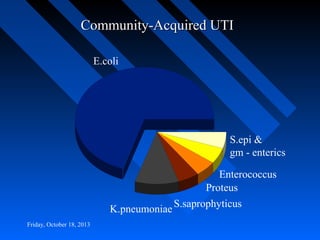
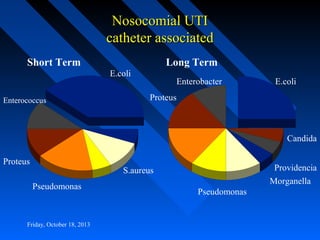
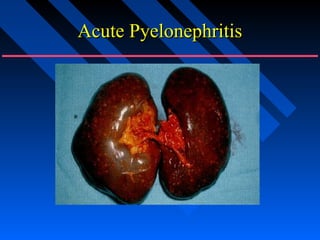
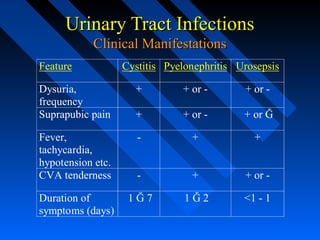
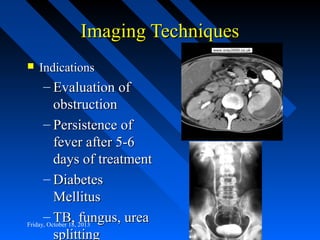
This document provides information on urinary tract infections (UTIs). It defines different types of UTIs and describes the signs of pyelonephritis. It discusses how to determine if a urine culture is positive and what imaging may be needed. The document emphasizes the importance of early diagnosis and prompt treatment of UTIs. It describes the typical causative organisms of community-acquired and nosocomial UTIs. Signs and symptoms of cystitis are outlined. Treatment recommendations include common antibiotic options and duration of treatment for UTIs.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














