Complicated and uncomplicateduti
Uncomplicated UTI-
Infection occurs in a structurally and functionally normal urinary tract.
Usually affects healthy, non-pregnant, premenopausal women.
• Pathogens are typically E. coli and prognosis is good with short-
course therapy.
• Complicated UTI-
• Infection occurs in urinary tracts with structural/functional
abnormalities (e.g., obstruction, catheter, stones, neurogenic
bladder).
• Occurs in men, pregnant women, or immunocompromised/
hospitalized patients.
• Broader range of organisms, higher risk of resistance, recurrence,
and treatment failure.
3.
Indications for hospitalisationfor complicated uti
Septic or critically ill patient
persistently high fever (eg, >38.4°C/>101°F) or pain marked
debility,
inability to maintain oral hydration or take oral medications.
Suspected urinary tract obstruction
• Other patient with uncomplicated UTI and acute
complicated UTI of mild to moderate severity who can be
stabilized can be managed in outpatient basis or emergency
department and discharged on oral antimicrobials with
close follow-up.
4.
Contd ..
• Treatmentshould be started immediately and modified if
nec- essary when the bacteriological report is to hand.
• The treatment is started with the antibiotics
• Failure to respond indicates the need for further
investigation to exclude predisposing factors
• It is important to check for associated allergies or other
drugs or conditions that might preclude the use of some
antibiotics
6.
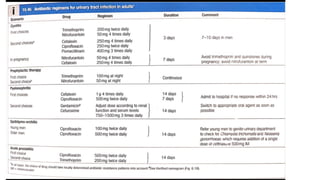
Antimicrobial in pregnancy
Nitrofurantoin,ampicillin, and the cephalosporins are considered relatively
safe in early pregnancy.
Sulfonamides should clearly be avoided both in the first trimester (because
of possible teratogenic effects) and near term (because of a possible role in
the development of kernicterus).
Fluoroquinolones are avoided because of possible adverse effects on fetal
cartilage development.
• Pregnant women with ASB are treated for 4-7 days. With overt
pyelonephritis, parenteral ẞ-lactam therapy with or without
aminoglycosides is the standard of care.
7.
Patients on catheters
Donot rely on classical clinical symptoms or signs for
predicting the likelihood of symptomatic UTI in catheterised
patients.
Signs and symptoms compatible with catheter-associated
UTI include:
new onset or worsening of fever, rigors
altered mental status, malaise, or lethargy
flank pain or costovertebral angle tenderness
• acute haematuria
8.
Management of patientswith
catheters
Do not use dipstick testing to diagnose UTI in patients with
catheters.
Antibiotic treatment
Do not treat catheterised patients with asymptomatic
bacteriuria with an antibiotic.
• Do not routinely prescribe antibiotic prophylaxis to prevent
symptomatic UTI in patients with catheters.
9.
Response to therapy
Iftherapy is appropriate, clinical response should occur within 24
hours with treatment of cystitis.
With pyelonephritis, response should occur by 48 to 96 hours.
Lack of response by 72 hours should be an indication for imaging
studies.
Four patterns of response of bacteriuria to antimicrobial therapy-
cure, persistence, relapse, and reinfection
Bacteriologic Cure is defined as negative urine cultures on
chemotherapy and during the follow-up period, usually 1 to 2 weeks.
• Bacteriologic Persistence- It is persistence of significant bacteriuria
after 48 hours of treatment. Causes are the urinary levels of the
drug are inordinately low (i.e., from not taking the agent,
insufficient dosage, poor intestinal absorption, or poor renal
excretion, as in renal insufficiency or resistent strain.
10.
Relapse and reinfection
IfUTI is recurrent it is necessary to distinguish between relapse and
reinfection.
Relapse is diagnosed by recurrence of bacteriuria with the same
organism within 7 days of completion of antibacterial treatment and
implies failure to eradicate infection usually in conditions such as
stones, scarred kidneys, polycystic disease or bacterial prostatitis.
• Reinfection is when bacteriuria is absent after treatment for at least
14 days, usually longer, followed by recurrence of infection with the
same or different organisms. This is the result of reinvasion of a
susceptible tract with new organisms. Approximately 80% of
recurrent infections are due toreinfection
11.
Non microbial therapy
Ahigh (2 L daily) fluid intake is encouraged during treatment
Drinking too much water can worsen the symptoms in few
conditions
• To acidify the urine, it is often necessary to modify the diet
by restriction of agents that tend to alkalinize the urine (e.g.,
milk, fruit juices
• Cranberry juice – disable the ability of E. coli to adhere to the
epithelial cells of the urethra.
12.
Surgical management
Surgery isnever directed at the infection alone, but at removing the
underlying cause (obstruction, abnormality, or complication).
• Antibiotics are given first; surgery follows once sepsis is controlled.
13.
Contd…
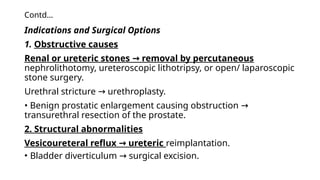
Indications and SurgicalOptions
1. Obstructive causes
Renal or ureteric stones removal by percutaneous
→
nephrolithotomy, ureteroscopic lithotripsy, or open/ laparoscopic
stone surgery.
Urethral stricture urethroplasty.
→
• Benign prostatic enlargement causing obstruction →
transurethral resection of the prostate.
2. Structural abnormalities
Vesicoureteral reflux ureteric
→ reimplantation.
• Bladder diverticulum surgical excision.
→
14.
Contd…
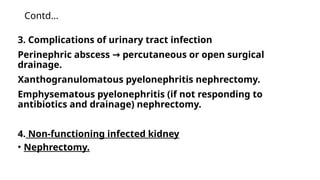
3. Complications ofurinary tract infection
Perinephric abscess percutaneous or open surgical
→
drainage.
Xanthogranulomatous pyelonephritis nephrectomy.
Emphysematous pyelonephritis (if not responding to
antibiotics and drainage) nephrectomy.
4. Non-functioning infected kidney
• Nephrectomy.

































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)