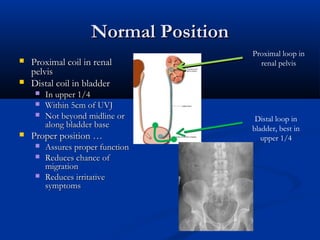
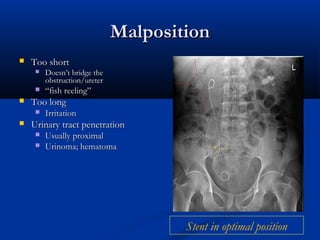
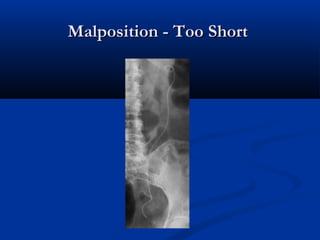
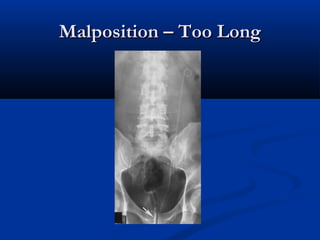
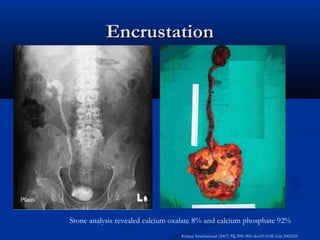
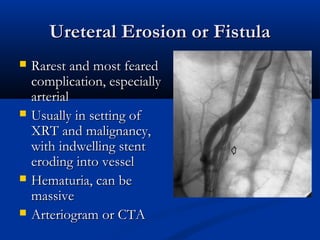
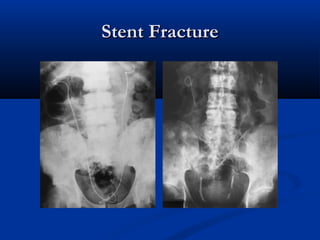
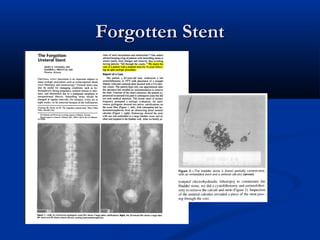
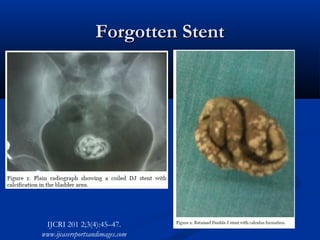
Ureteral stents are used to relieve benign or malignant obstruction of the ureter or as an adjunct to stone therapy. They are typically placed cystoscopically with the proximal coil in the renal pelvis and distal coil in the bladder. Complications can include malposition if too short or long, migration, urinary tract infection, inadequate relief of obstruction, encrustation, fracture, or erosion of the ureter. Careful positioning and timely removal are important to prevent complications.
































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







