2
Objectives
At theend of this unit learners will be able to:
1. Define the Urinary System.
2. List the organs of Urinary system
3. Discuss the location of the kidney.
4. Discuss kidneys in terms of external anatomy, gross structure &
microscopic structure.
5. Describe the role of each component of nephron in terms of filtration,
selective reabsorption & secretion involved in the formation of urine.
6. Briefly discuss the role of kidney in maintaining water and electrolyte
balance.
7. Discuss the structure and functions of:
• Ureters
• Urinary bladder
• Urethera
8. Briefly explain the process of micturation
3.
3
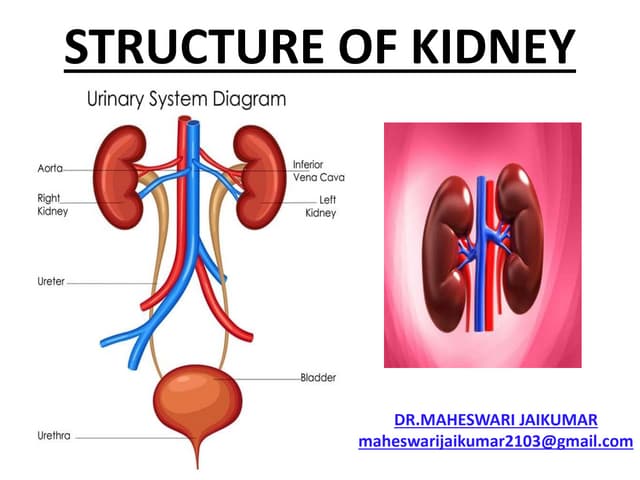
Urinary System:
• Asystem that produces, stores, and excretes
urine via a filtration mechanism in which
potentially harmful molecules are removed
from the body.
• It also plays a crucial role in water homeostasis,
electrolyte - acid-base balance and red blood
cell production.
• Comprised of two kidneys, two ureters, one
bladder, two sphincters, and one urethra.
4.
4
cont
• Urology :The branch of medicine that deals with the
male and female urinary systems and the male
reproductive system.
• Nephrology : the scientific study of the anatomy,
physiology, and pathology of the kidneys.
• Nephrologists: specialist that treats diseases that
affect the kidneys function ; such as diabetic
neuropathy , kidney failure.
• Urologists : specialist who treats conditions of the
urinary tract, including those that can be affected by
the kidneys: such as kidney stones and obstruction.
6
Functions
1. Kidneys regulateblood volume & composition:
help regulate blood pressure, pH & glucose level
Produce two hormones (calcitriol and
erythropoietin) enzyme (renin = helps to
regulate BP) and excrete wastes in urine.
2. Ureters transport urine from kidneys to urinary
bladder.
3. Urinary bladder stores urine and expels it into
urethra.
4. Urethra discharges urine from body.
7.
7
Kidneys Function
• Excretionof wastes: Some wastes excreted via urine
result from metabolic reactions;
Urea and ammonia from the deamination of amino
acids.
Creatinine from the breakdown of creatine
phosphate.
Uric acid from the catabolism of nucleic acids; and
Urobilin from the breakdown of hemoglobin.
o Nitrogenous wastes : Urea, ammonia, creatinine, uric
acid, and urobilin.
o Foreign substances ; such as drugs and environmental
toxins also excreted in urine.
8.
8
• Regulation ofblood ionic composition; kidneys help
regulate the blood levels of several ions, most
importantly sodium ions (Na+), potassium ions (K+),
calcium ions (Ca+2
), chloride ions (Cl−), and phosphate
ions (HPO4-2
).
• Regulation of blood pH: Excrete a variable amount of
hydrogen ions (H+) into the urine and conserve
bicarbonate ions (HCO3−), which are an important buff
er of H+ in the blood.
• Maintenance of blood osmolarity: By separately
regulating loss of
water and loss of solutes in the urine, the kidneys maintain
a relatively constant blood osmolarity close to 300
milliosmoles per liter (mOsm/liter).
9.
9
• Regulation ofblood volume; Adjust blood volume by
conserving or eliminating water in the urine. (An increase or
decrease in blood volume effects blood pressure).
• Regulation of blood pressure: the enzyme renin activates
the renin– angiotensin–aldosterone pathway (↑ of renin =
↑blood pressure).
Production of hormones; hormones: Calcitriol, the active form
of vitamin D, helps regulate calcium homeostasis and
erythropoietin stimulates the production of red blood cells.
• Regulation of blood glucose level: the kidneys can use the
amino acid glutamine in gluconeogenesis, the synthesis of
new glucose molecules, then release glucose into the blood
to maintain a normal blood glucose level.
10.
10
Kidney
• Bean shapedreddish-brown retroperitoneal organ.
• Located between peritoneum and the posterior wall of
the abdomen.
• At the level T12 & L 3 vertebrae, so partially protected
by ribs 11 and 12.
• Right kidney is slightly lower than the left (liver).
• Size: 10–12 cm (4–5 in.) long, 5–7 cm (2–3 in.) wide,
and 3 cm (1 in.) thick
About the size of a bar of bath soapand has a
• Mass / Weight: 135–150 g (4.5–5 oz)
11.
11
Organs associated withthe kidneys
Right kidney
• Superiorly – the right
adrenal gland
• Anteriorly – the right lobe
of the liver, the
duodenum & hepatic
flexure of the colon
• Posteriorly – diaphragm,
& muscles of posterior
abdominal wall.
Left kidney
• Superiorly : the left
adrenal gland
• Anteriorly – the spleen,
stomach, pancreas,
jejunum and splenic
flexure of the colon
• Posteriorly : diaphragm
and muscles of the
posterior abdominal wall.
12.
12
External Anatomy
• Concavemedial border faces the vertebral column( hilum ).
• Renal hilum : Near the center of the concave border; the ureter emerges
from the kidney along with blood vessels, lymphatic vessels, and nerves.
• Three layers of tissue surround each kidney .
The deep / internal layer, (renal capsule): a smooth, transparent sheet
of dense irregular connective tissue that is continuous with the outer
coat of the ureter; serves as a barrier against trauma and helps maintain
the shape of the kidney.
The middle layer, (adipose capsule) : a mass of fatty tissue surrounding
the renal capsule. It also protects the kidney from trauma and holds it
firmly in place within the abdominal cavity.
The superficial layer, (the renal fascia): thin layer of dense irregular
connective tissue that anchors the kidney to the surrounding structures
and to the abdominal wall, it is deep to the peritoneum at anterior
surface of kidneys.
14
Internal Anatomy ofthe Kidneys
A frontal section reveals two distinct regions:
• The renal cortex : a superficial, light red region; the smooth-
textured area extending from the renal capsule to the bases of
the renal pyramids and into the spaces between them (column).
It is divided into an outer cortical zone and an inner
juxtamedullary zone.
• The renal medulla (medulla = inner portion): deep, darker
reddish-brown inner region, consists of several cone-shaped
structures renal pyramids (16 - 18).
The base (wider end) of each pyramid faces the renal cortex, and
its apex (narrower end / a renal papilla, points toward the renal
hilum).
• The parenchyma : or functional portion of the kidney, developed
by , the renal cortex and renal pyramids of the renal medulla.
15.
15
Nephrons.
• Nephrons: microscopicstructures and functional units
of the kidney within the parenchyma (about 1 million)
Filtrate (filtered fluid) drains into large papillary ducts,
which extend through the renal papillae of pyramids.
The papillary ducts drain into minor and major calyces
(singular is calyx = cuplike structures ); pronounced
Kidney has 8 to 18 minor and 2 or 3 major calyces.
Major Calyx drain filtrate(urine) into pelvis.
• Renal sinus; a cavity in which hilum expands
16.
16
Renal pelvis
• Abasin, funnel shaped
collects the urine via
Major calyces.
• Walls contain smooth
muscle and lined with
transitional epithelium.
• Helps to form the
upper end of the
ureters.
• Edges of the renal
pelvis closest to the
renal pyramids calyce.
20
Nephron
• A nephronis functional unit of a kidney, having two main parts
1. Renal corpuscle: Filtration of blood
• The head of the nephron
(a) The renal corpuscle is composed of Bowman’s capsule and
glomeruli
(b) Bowman’s capsule is the cover of the corpuscle that surrounds
the glomerulus
(C) The glomerulus ; network of capillaries found inside corpuscle.
2. Renal tubule: Reabsorption and secretion.
The tubular passageway of the nephron & described in three parts.
• Proximal convolutes tubule (PCT)
• Loop of Henle
• Distal convoluted tubule (DCT)
23
Differences between cortical& juxtamedullary NEPHRONS
a) CORTICAL
• Form 80% of total
nephrons.
• Are small in size.
• bowman’s capsule in
the cortex
• Henle’s loops are very
short and extend only
a little into the
medulla.
• Do not have vasa racta.
(b) Juxtamedullary
• Form only 20% nephrons
• Are in large in size.
• bowman’s capsule in the cortex
• Henle’s loops are very long and extend.
• Vasa racta are present.
it enters the medulla where the solute
concentration in the interstitium is
high.
It acts with the loop of Henle to
concentrate the urine
If the vasa recta did not exist, the high
concentration of solutes in the
medullary interstitium would be
washed out.
25
Renal Glomerulus
• tightly-coiledcapillaries network.
• It performs the first step of filtering blood.
• Operates as a nonspecific filter - removes both useful
and non-useful material.
• The endothelial cells are fenestrated
(pores/transparent areas).
• The walls of the glomerulus and the glomerular capsule
consist of a single layer of flattened epithelial cells.
• The glomerular walls are more permeable than those
of other capillaries.
26.
26
Layers of Glomerulus(filtration membrane)
1. Endothelial cells :
• The endothelial cells of the glomerulus contain
numerous pores called fenestrate.
• These pores are relatively large, they allow for the
free filtration of fluid, plasma solutes and
protein.
2. Glomerular basement membrane:
• A fusion of the endothelial cell and podocyte basal
laminas(specialized epithelial cells /outer
surfaces of glomerular capillaries)
3. Podocytes :
• Podocytes line the other side of the glomerular
basement membrane and form part of the lining
of Bowman's space.
• Podocytes form a tight pedicels that control the
filtration of proteins, and clefts between them
called slits.
27.
27
Bowman’s Capsule
• Itis double walled cup-shaped.
• A sac that encloses glomerulus
• It receives the fluid filtered at the
glomerulus
• Transfers filtrate from the glomerulus
to the Proximal Convoluted Tubule
(PCT).
Divided into two layers
• Parietal or capsular layer - simple
squamous epithelium.
• Visceral layer – podocytes
Bowman's space: the space between the
capillary tuft and Bowman’s capsule.
Bowman’s space
28.
28
Renal tubule
Tubule (PCT)(Proximal Convoluted Tubule)
• The proximal tubule leads from the Bowman’s capsule to the
Loop of Henle.
• It lies in the renal cortex.
• PCT is lined by cuboidal epithelial having brush borders with long
microvillus for increasing absorptive area.
• PCT reabsorbs about 65% of the glomerular filtrate and return it
to the blood.
• Reabsorbs most of the useful substances of the filtrate:
sodium (65%), water (65%), bicarbonate (90%), chloride (50%),
glucose(nearly 100%)
• The primary site for secretion (elimination) of drugs, waste and
hydrogen ions.
30
Nephron structures andfunctions
The loop of Henle
• U-shaped long tube loop which extends into the medulla that consists of:
Descending limb of loop of Henle
Ascending limb of loop of Henle
• Its primary role is to concentrate the salt in the interstitium, the tissue
surrounding the loop.
Descending Limb of the Loop of Henle
• Fully permeable to water and completely impermeable to solutes (salt particles)
• receives filtrate from the PCT, allows water to be absorbed and passes “salty”
filtrate to the next segment. “Saves water and passes the salt”
Ascending Limb of the loop of Henle
• impermeable to water and actively transports (reabsorbs) salt (NaCl) to the
interstitial fluid of the pyramids in the medulla. “Saves salt /passes the water.”
• the passing filtrate becomes dilute
31.
31
Juxtaglomerular apparatus
Juxtaglomerular apparatusis
part of kidney nephron,
next to the glomerulus.
• It is found between where
blood enters a renal
corpuscle and the distal
convoluted tubule of the
same nephron.
• The juxtaglomerular
apparatus consists of the
• Macula densa,
• Juxtaglomerular cells,
32.
32
Cont…
• Juxtaglomerular cells(JGC) lie in the wall of afferent
arteriole, specialized smooth muscle, which supplies
blood to the glomerulus.
Act as mechanoreceptors that sense blood pressure low,
then release renine.
Function: Secrete –Renin (an angiotensinogenase):
convert angiotenosin into angiotensin-I.
• Macula densa modified epith. cells in initial portion
of DCT Function : sense change of volume and NaCl
concentration of tubular fluid , and transfer information
to JGC.
33.
33
Cont..
Distal Convoluted Tubule(DCT)
• It is highly coiled part of
nephron
• Receives dilute fluid from the
ascending limb of the loop of
Henle.
• Gets rid of those substances
the body doesn’t want or
need; reabsorbs some more
Na+, Ca2+.
• Fine control of blood
composition.
Collecting Duct
• The last segment to save
water for the body.
• Regulate water contents
of body fluid
(osmoregulation) (ADH)
34.
34
Physiology of UrineFormation
• Kidney form urine by
three precisely regulated
processes
1) Ultrafiltration
2) Tubular Reabsorption
3) Tubular Secretion.
4) Excretion
35.
35
1. Ultrafiltration (glomerularfiltration)
• High pressure filtration via
semipermeable membrane in
which colloidal particles are
retained while the small
sized solutes and the solvent
are forced to move across the
membrane by hydrostatic forces.
• Plasma proteins, cellular
components not filtered.
• Some drugs amount may not filter
such as; penicillin and aspirin.
36.
36
Constituents of glomerularfiltrate & glomerular capillaries
Blood constituents in glomerular filtrate
• Water
• Mineral salts (Na+
, Cl−
, Mg2+
, Ca2+
,H, K+)
• Amino acids
• Keto acids
• Glucose
• Some hormones
• Creatinine
• Urea
• Uric acid
• Some drugs (small molecules)
All content of plasma filtered except plasma
proteins.
99% of filtrate are reabsorbed and less than
1 % only form urine.
Constituents
remaining in
glomerular
capillaries
• Leukocytes
• Erythrocytes
• Platelets
• Plasma proteins
• Some drugs (large
molecules)
37.
37
Renal plasma flow(RPF/GFR)
Volume of plasma flow in both kidneys per minutes.
• Kidneys have a very high blood flow
• 20% of cardiac output (5 to 6 L/min) i.e, about 1.2
L/min.
• 1/5th
of cardiac out/min i.e.= 1000-1200ml
600 - 650ML/min (Plasma (55%) approx: 650ml)
Renal plasma flow= 55% of 1000- 1200 ml/min
= approximately 600ml/ min.
Filtration fraction: GFR/RPF % (normal eGFR > 90 %)
Approximately 20% of plasma as filtered & rest go forward
into efferent arteriole.
39
Glomerular Filtration Rate.(GFR)
•Thevolume of filtrate formed by both kidneys each
minutes is called GFR.
•The normal rate is 125mL/min
125* 60 = 7500mL/hr
7500* 24 = 180L/day both kidneys. 180/3 = 60
Plasma volume (70-kg young adult man) = about 3L, the
kidneys filter the plasma some 60 times in a day.
About 99% filtrate is absorbed and about 1 % (1 – 1.5 l)
excreted
40.
40
Glomerular Filtration Process
•One pressure promotes filtration
• Two pressures oppose filtration
1. Glomerular blood hydrostatic pressure – 55 mmHg / 7.3 kPa.
• Promotes filtration by forcing water and solutes through filtration
membrane.
2. Capsular hydrostatic pressure(CHP) –15 mmHg/4 kPa
• Opposes filtration by exerting back pressure against filtration
membrane.
3. Blood colloid osmotic pressure(BCOP) – 30 mmHg/2 kPa
• Opposes filtration by the presence of proteins in blood plasma
which slows down osmosis.
• Changes to either of these three pressures will affect the
Glomerular Filtration Rate (GFR)
42
Control of FiltrateRate
• GFR remains relatively constant through a
process called auto-regulation
• Certain conditions override auto-regulation,
including when GFR increases
• Primarily three mechanisms are responsible
for keeping the GFR constant:
Renal Autoregulation
Neural regulation
Hormonal regulation
43.
43
Control of FiltrateRate/ Kidney Function
Intrinsic mechanisms:
• Renal autoregulation
Adjust their own blood flow and GFR without external control
(nervous, hormonal) .
Renal blood flow is maintained at a constant pressure across a wide
range of systolic blood pressures (from around 80–200 mmHg).
• May be stimulated by changes in blood pressure in the renal
arteries or by fluctuating levels of certain metabolites, e.g.
prostaglandins.
It enables them to maintain a stable GFR even when BP rises.
Helps to ensure stable fluid and electrolyte balance.
• In severe shock, (BP falls < 80 mmHg) , autoregulation fails and
renal blood flow and the hydrostatic pressure decrease, impairing
filtration within the glomeruli.
44.
44
Cont…
Extrinsic mechanisms:
• Neural(nervous system) control : (RAAS) (work < BP)
- Override renal autoregulation and decrease the glomerular
filtration rate when necessary.
• Stimulate contraction of the afferent arteriole, reducing urine
production.
• It can also activate the renin-angiotensin-aldosterone system, a
hormone system that regulates blood pressure and fluid balance
when needed.
• Hormonal control - atrial natriuretic peptide (inhibit the
release of renin); It can increase the glomerular filtration
rate. This hormone is produced in heart and is secreted when
plasma volume increases, which increases urine production.
48
2. Reabsorption
Selective reabsorption
•Na+
, K+
, P4 Ca+
• Cl
• Glucose
• Amino acids
• Urea
• Bicarbonate
• Water (osmosis)
Active
absorb
Passive /
Diffusion
Re absorption of the nitrogenous substances: urea, uric acid and creatinine is very
limited and glucose, amino acids totally absorbed unless excess in blood
49.
49
Tubular Reabsorption
Selective reabsorption
•PCT : proximal convoluted tubule:
Many substances are reabsorbed
here; some water, electrolytes and
organic nutrients (glucose) 30 – 40 %
Descending Limb Loop of Henle ( 50%)
• Fully permeable to water and
completely impermeable to solutes
(salt particles)
Ascending Limb of loop of Henle (15 – 20
%)
• Impermeable to water and actively
transports (reabsorbs) salt (NaCl)
Thick loop of Henle; Reabsorb: Na+
, Cl−
,
Mg2+
, Ca2+
, K+
50.
50
Cont…
Reabsorption in EarlyDCT
• Absorb 10-15% of water and 5% of Na+ and Cl-
• Also where parathyroid hormone (PTH) stimulates reabsorption of
Ca2+ depending on body’s needs.
Reabsorption in late DCT &
Collecting Ducts
• Filtrate inthe collecting ducts is quite dilute and duct reabsorb as
much
water as the body needs.
• Cells in the collecting duct make the final fine tuning adjustments:
principal cells reabsorb Na+ and secrete K+; facultative reabsorption
of H2O (ADH)
intercalated cells(epithelial cells) reabsorb K+ & bicarbonate ions
(HCO3) and secrete H+ (regulate pH)
51.
51
Hormones influence selectivereabsorption
• Angiotensin II; Leads to vascular resistance that > BP
• Aldosterone; increases the reabsorption of sodium and water,
and the excretion of potassium.
• Atrial natriuretic peptide (ANP) : secrested when blood volume
increases, It leads decrease in reabsorption of sodium and water
from the proximal convoluted tubules and collecting ducts.
• Antidiuretic hormone (ADH) : increases the permeability of the
distal convoluted tubules and collecting tubules so increasing
water reabsorption.
• Parathyroid hormone (PTH): secreted together with calcitonin &
regulates the reabsorption of calcium and phosphate from the
distal collecting tubules.
• AS PTH increases the blood calcium & calcitonin decreases.
52.
52
3. Secretion
• Thesubstances are not filtered are cleared by
secretion from the peritubular capillaries into the
filtrate within the convoluted tubules.
• Tubular secretion of hydrogen ions (H+) is important in
maintaining normal blood pH.
• Ensure that wastes such as creatinine, urea, excess H+
& K+ ions are actively secreted into the filtrate.
• Secretion plays a crucial role in maintaining the body's
ACID-BASE BALANCE.
• The tubular filtrate is finally known as urine.
• Human urine is usually hypertonic.
53.
53
Cont…
• K+
plasma concentrationis 3.5 -5.0 mmol/L.
mmol = Millimoles per litre
• Ca+
plasma level is 2.2-2.6 m mol/lit
• A normal serum Cl concentration is 98-108 mmol/L.
• Na+
concentration is 134-145 mmol/L.
• HCO3 serum concentration is 22-30 mmol/L.
• Phosphate plasma concentration 1.7 – 2.6 mEq/litre.
milliequivalents per litre = mEq/l
54.
54
Excretion
• Process ofexcretion of waste (water &
chemical substance ) via collecting ducts up to
bladder & Urethra
55.
55
Transport Maximum orRenal Threshold
• It is a kidneys’ maximum capacity for
reabsorption of a substances.
• For example, the normal blood glucose level is
3.5–8 mmol/L (63 to 144 mg/100 mL) and if this
rises above the transport maximum of about 9
mmol/L (160 mg/100 mL), glucose appears in
the urine.
56.
56
Composition of Urine
•Urine is clear and amber (yellow) in colour due
to the presence of urobilin (bile pigment,
reabsorbed & excreted by kidneys).
• Specific gravity ; 1020 – 1030.
• pH is around 6 (normal range 4.5–8).
• Normal Volume(adult) : 1000 to 1500 mL / day
• Minimum volume : about 500 mL per day.
58
Factors influence onthe urine volume
– Intake of fluid, proteins and salt.
– Excessive perspiration and strenuous exercise
_Long standing urine may become turbid. (Due to
precipitation of phosphates).
_High protein diet makes the urine more acidic
– Diet rich in vegetables/ fruits make urine more alkaline
• Excessive urine output is called polyuria.
• Scanty urine output is oliguria (output of less than 400
mL/day ) is insufficient to excrete toxic wastes.
• Pyuira : Pus in urine
• No urine : Anuria
60
Nephroptosis
• The floatingkidney, is an inferior displacement
or dropping of the kidney.
Most often in very thin people whose adipose
capsule or renal fascia is deficient.
Dangerous because the ureter may kink and
block urine flow, results backup of urine puts
pressure on the kidney, which damages the
tissue.
• Twisting of the ureter also causes pain
• 10 times more common in females than males.
61.
61
Ureters
• Muscular tubesleading from the
renal pelvis to bladder.
• About 25 to 30 cm (10 – 12 inches)
long with a diameter of about 3 mm
• Extends downward posterior to the
parietal peritoneum.
• Runs parallel to vertebral column
• Join the urinary bladder in the pelvic
cavity
• Ureter wall has three layers:
The inner mucous coat
(transitional epithelium)
The middle muscular coat
(smooth muscles fibers)
The outer fibrous coat
(connective tissue)
Lumen
Mucous coat
Muscular coat Fibrous coat
Adipose tissue
62.
62
Function of Ureters
•Propel urine into the bladder by peristaltic
contraction of the smooth muscle layer.
• It is intrinsic property of the smooth muscle and
is not under autonomic nerve control.
• Peristalsis originates in a pacemaker in the
minor calyces.
• Peristaltic waves occur several times per
minute, increasing in frequency with the
volume of urine produced, sending little spurts
of urine into the bladder.
63.
63
Urinary Bladder
• Ahollow, distensible, muscular organ located within pelvic cavity, posterior to symphysis pubis & inferior to
parietal peritoneum
• Contacts the anterior walls of the uterus and vagina in the female, and lies posteriorly against the rectum
in the male.
• It has a folded internal lining (known as rugae), which allows it to accommodate up to 400-600ml of urine
in healthy adults.
• Internal urethral sphincter:
Male – consists of circular smooth fibres, which are under autonomic control. It is thought to prevent seminal
regurgitation during ejaculation.
Females – thought to be a functional sphincter (no sphincteric muscle present). It is formed by the anatomy of
the bladder neck and proximal urethra.
• External urethral sphincter – has the same structure in both sexes. It is skeletal muscle, and under
voluntary control.
Mmales the external sphincteric mechanism is more complex, as it correlates with fibers of the
rectourethralis muscle and the levator ani muscle.
64.
64
External Features
• Apex– located superiorly, pointing towards the
pubic symphysis, It is connected to the
umbilicus by the median umbilical ligament.
• Body – main part of bladder, b/w apex & fundus
• Fundus (or base) – located posteriorly. It is
triangular-shaped.
• Neck – formed by the convergence of the
fundus and the two inferolateral surfaces. It is
continuous with the urethra
66
Cont…
• Trigone ;A triangular area on the bladder floor openings of the two ureters and
the urethra.
• It has three layers:
Inner Mucosa and submucosa coat ,
a muscular coat (detrusor muscle), and
an outer serous coat (Adventia).
• Smooth muscle fibers comprise the detrusor muscle which is the muscle of the
bladder wall.
• The detrusor muscle remains relaxed to allow the bladder to store urine, and
contracts during urination to release urine.
• The bladder stores urine - 400 to 600 ml
• Desire to urinate usually at 150ml.
• 300ml or more the sensation of fullness becomes increasingly uncomfortable.
• urine comfortably for 2 to 5 hours.
67.
67
• Arterial supply:the
superior vesical branch of
the internal iliac artery.
• Venous drainage:vesical
venous plexus, which
empties into the internal
iliac veins.
68.
68
Micturition;
The process oftime to time collection and removal of urine from
urinary bladder is known as micturition.
Sympathetic nerve: hypogastric nerve (T12 – L2).
relaxation of the detrusor muscle
Parasympathetic nerve
pelvic nerve (S2-S4); contraction of
detrusor muscle, stimulating micturition.
External sphincte (somatic control):
pudendal nerve (S2-4). innervates the external urethral sphincter, providing
voluntary control over micturition
.
sensory (afferent) nerves that report to the brain. They are found in the bladder
wall and signal the need to urinate when the bladder becomes full.
69.
69
Urinary Problems
• Problemswith detrusor muscle can lead to
incontinence. it is inability to control
urination, and is more common in women
than men.
• Urinary retention refers to the inability to
urinate.
• Nocturnal Enuresis = incontinence during the
night
70.
70
The Bladder StretchReflex
• It is a primitive spinal reflex, in which micturition is stimulated in response to
stretch of the bladder wall. It is analogous to a muscle spinal reflex, such as the
patella reflex.
• During toilet training in infants, this spinal reflex is overridden by the higher
centres of the brain, to give voluntary control over micturition.
Reflex ARC:
• Bladder fills with urine, and the bladder walls stretch. Sensory nerves detect
stretch and transmit this information to the spinal cord.
• Interneurons within the spinal cord relay the signal to the parasympathetic
efferents (the pelvic nerve).
• The pelvic nerve acts to contract the detrusor muscle, and stimulate
micturition.
• Although it is non-functional post childhood, the bladder stretch reflex needs
to be considered in spinal injuries (where the descending inhibition cannot
reach the bladder), and in neurodegenerative diseases (where the brain is
unable to generate inhibition).
71.
71
Urethra
• The urethrais a tube that conveys urine from the urinary bladder to the outside of
the body and also a reproductive function in the male, as a passage for sperm.
• Its wall is lined with a mucous membrane and it has a thick layer of longitudinal
smooth muscle fibers
• In a female:
• It is about 4 centimeters long (greater risk of urinary tract infections)
• It runs obliquely
• In a male:
• It is about 17.5 centimeters long
• It has a dual function for both
urination and reproduction
• It has three sections:
• Prostatic urethra(2.5cm)
• Membranous urethra (2cm)
• Penile urethra (15cm long)
(Difficulty in voiding urine with enlarged) prostate
73
Urethra
• In bothsexes:
Sphincters (circular muscles)
regulate the flow of urine
from the bladder.
– Internal urethral sphincter
= in the beginning of
urethra smooth muscle
– not under our voluntary
control
– External urethral sphincter
= skeletal muscle – we can
control it
internal urethral
sphincter
external urethral
sphincter
74.
74
References
• 2014. Ross& Wilson Anatomy And Physiology In
Health And Illness, 12Th Ed. Text. Churchill
Livingstone.
• Tortora, G. J. (2017). Principles of Human
Anatomy and Physiology (15th
ed). New York:
Happer & Row.