Downloaded 18 times















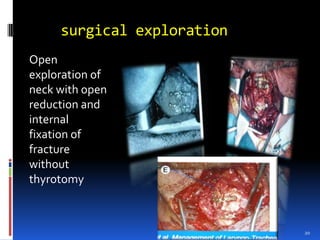
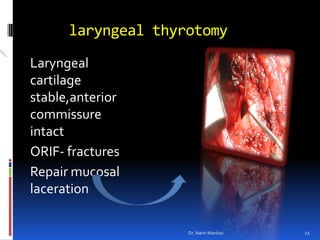






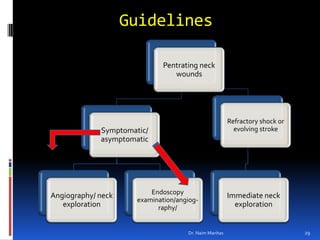
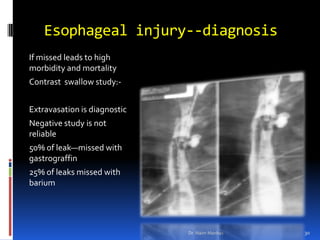



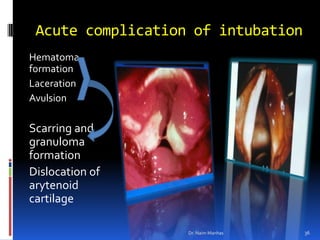
















Dr. Naim Manhas presented at the 4th Trauma Symposium on the management of laryngeal injuries in neck trauma. The presentation covered diagnosis and treatment of blunt and penetrating neck injuries, as well as iatrogenic laryngeal injuries from intubation. Complications from prolonged intubation can include hematoma, laceration, scarring, and limitation of vocal cord abduction. Prevention techniques aim to minimize intubation time and use proper tube size and positioning. Exploration is recommended for penetrating injuries in neck Zone 2 and those showing symptoms.























































































