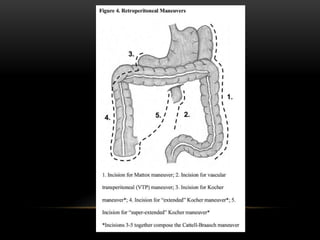
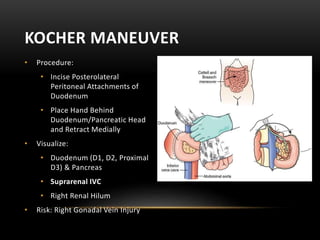
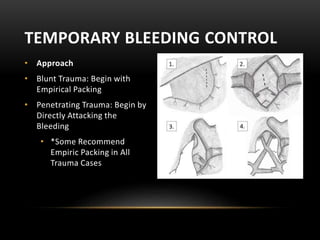
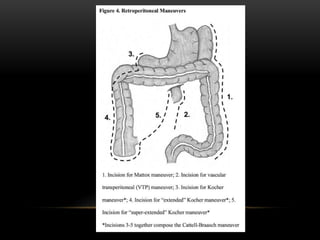
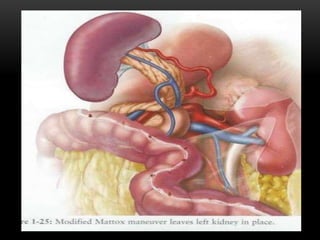
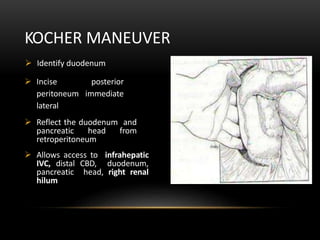
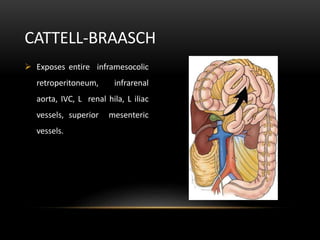
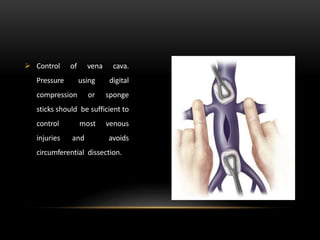
The document describes techniques for crash laparotomy in trauma patients. It discusses approaches for temporary bleeding control like packing and supraceliac aortic control. It also outlines the order of exploration as inframesocolic, supramesocolic, lesser sac, and retroperitoneum. Maneuvers like the Mattox maneuver and Kocher maneuver are explained to provide exposure and access during retroperitoneal exploration. The key decision of pursuing definitive repair versus damage control surgery is also covered, focusing on indications like severe physiologic insult or an injury pattern that would be difficult to assess or repair initially.






































































![[UPDATED] Kriteria 5 Keuangan 3A.docx](https://cdn.slidesharecdn.com/ss_thumbnails/updatedkriteria5keuangan3a-230528050724-387b130e-thumbnail.jpg?width=640&height=640&fit=bounds)
![List_ISO_Sabtu_28_Agustus_2021[1].docx](https://cdn.slidesharecdn.com/ss_thumbnails/listisosabtu28agustus20211-230525102109-88edaad6-thumbnail.jpg?width=640&height=640&fit=bounds)

























