



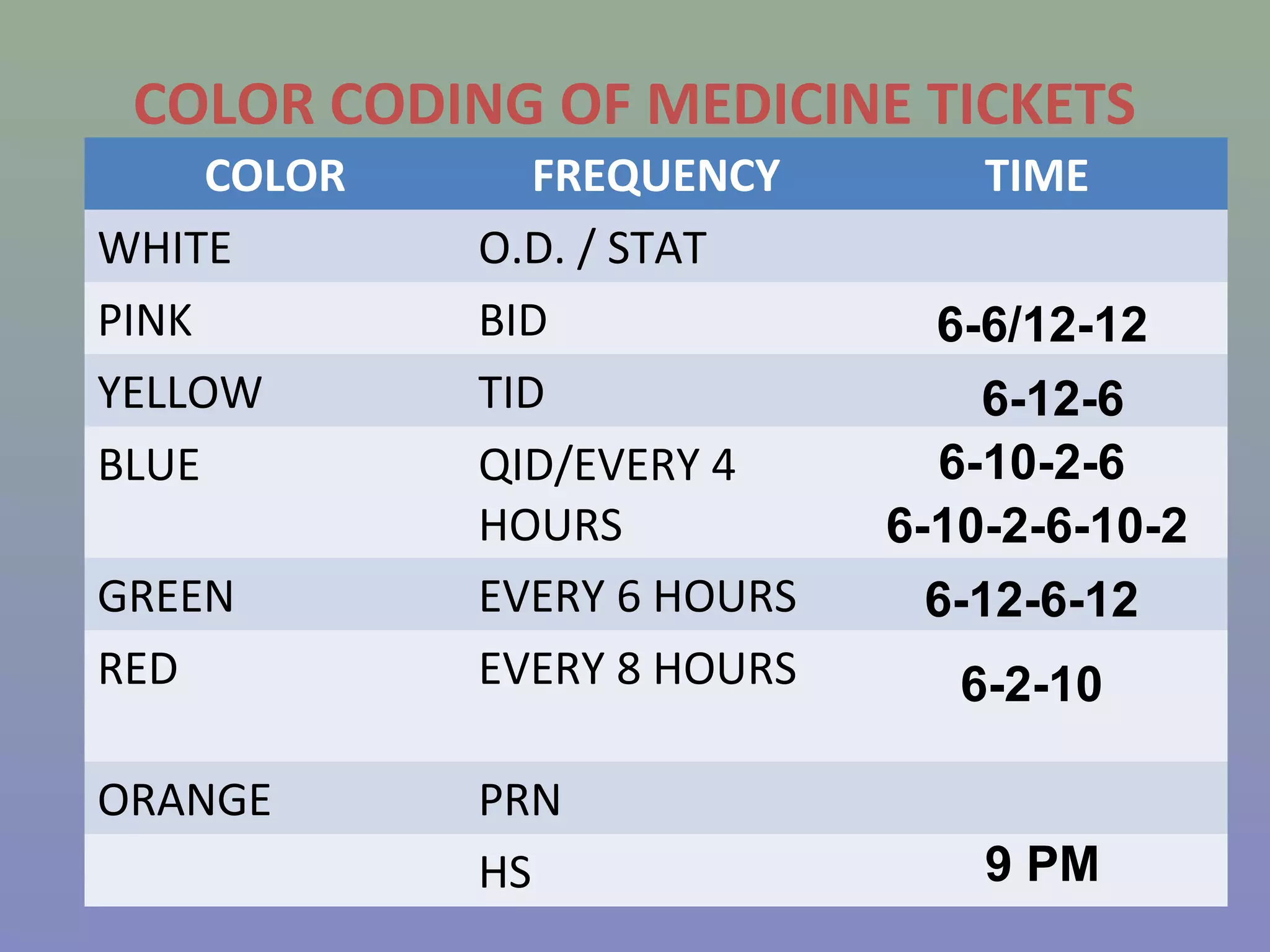
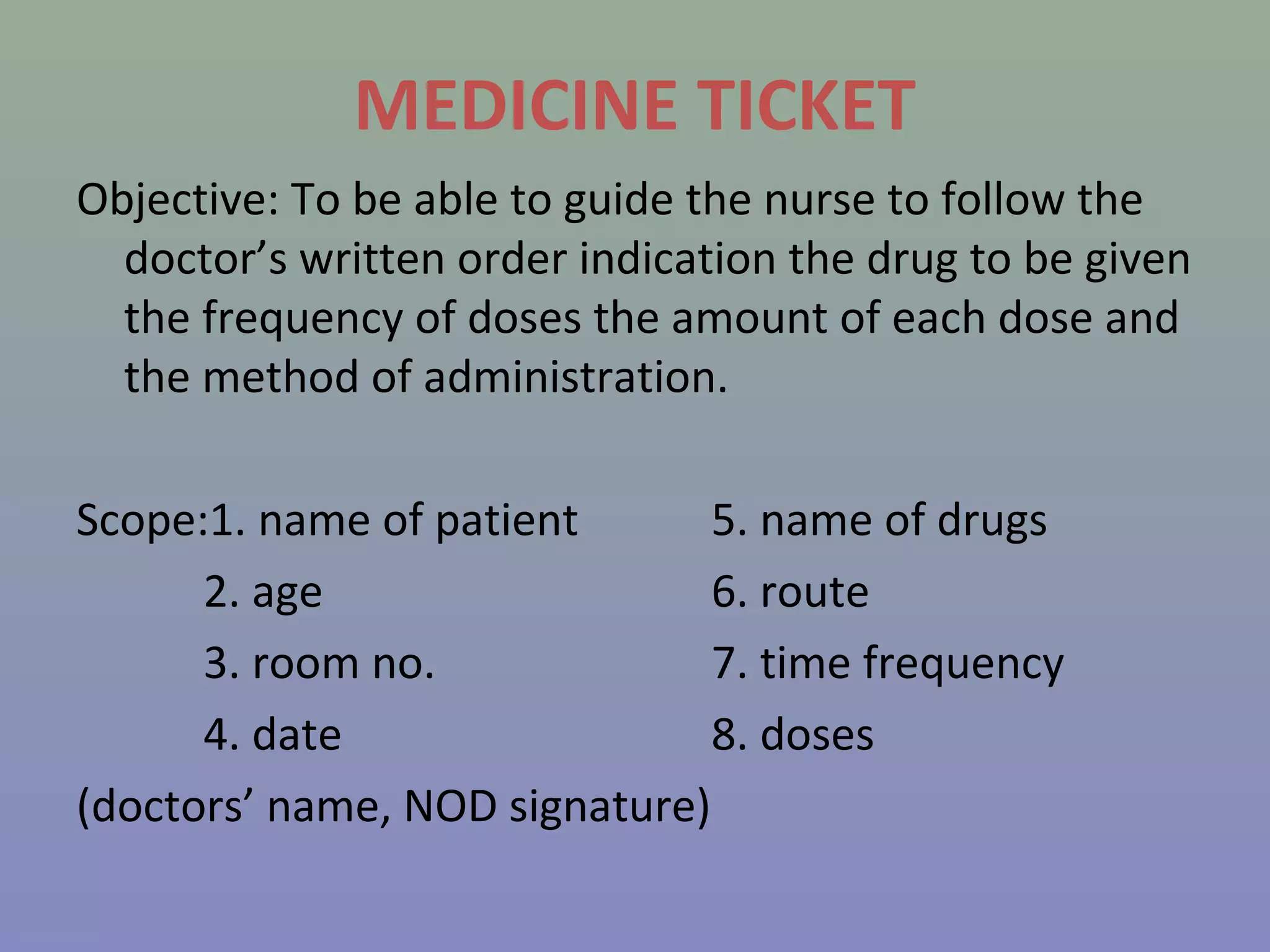
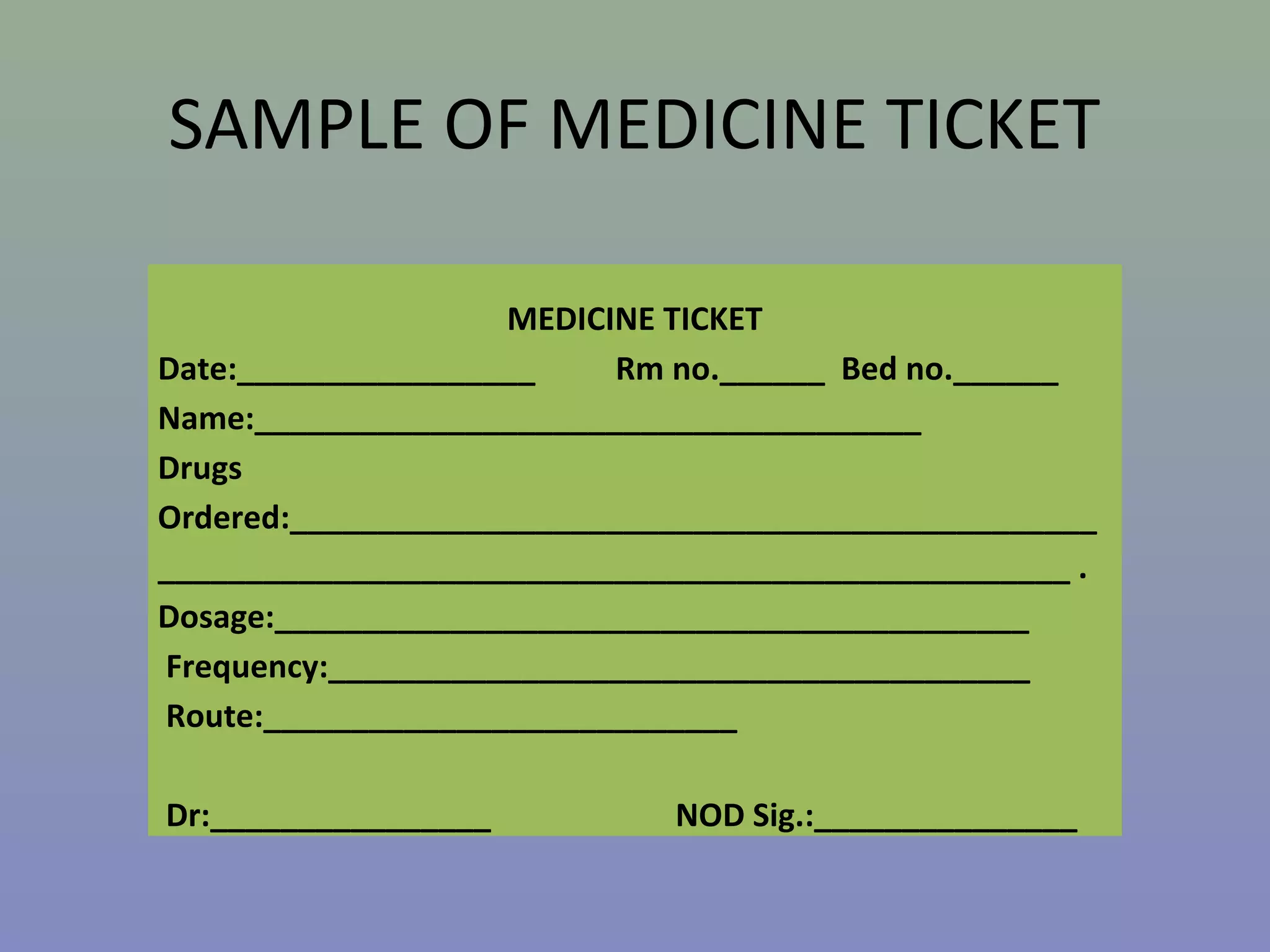
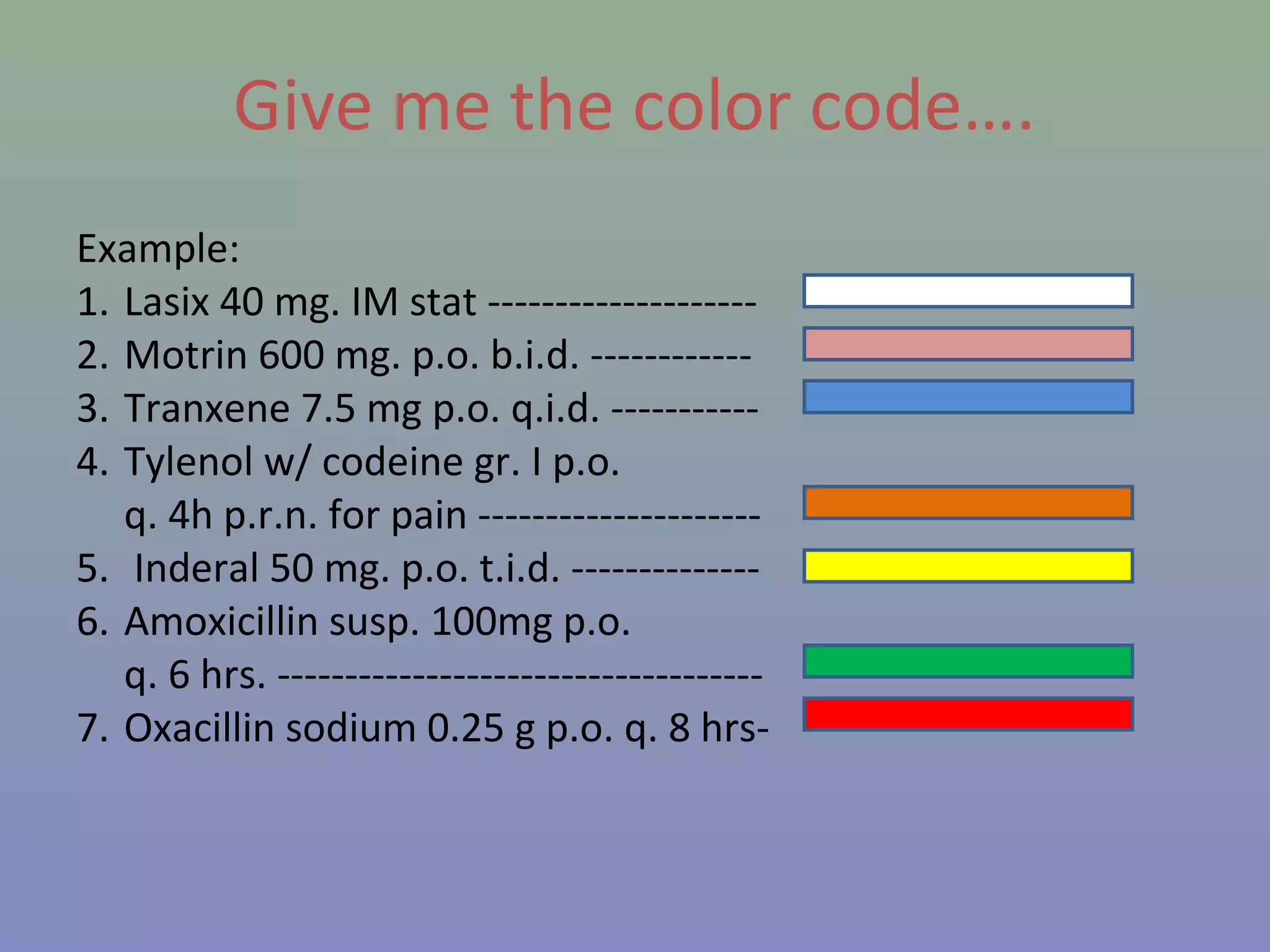
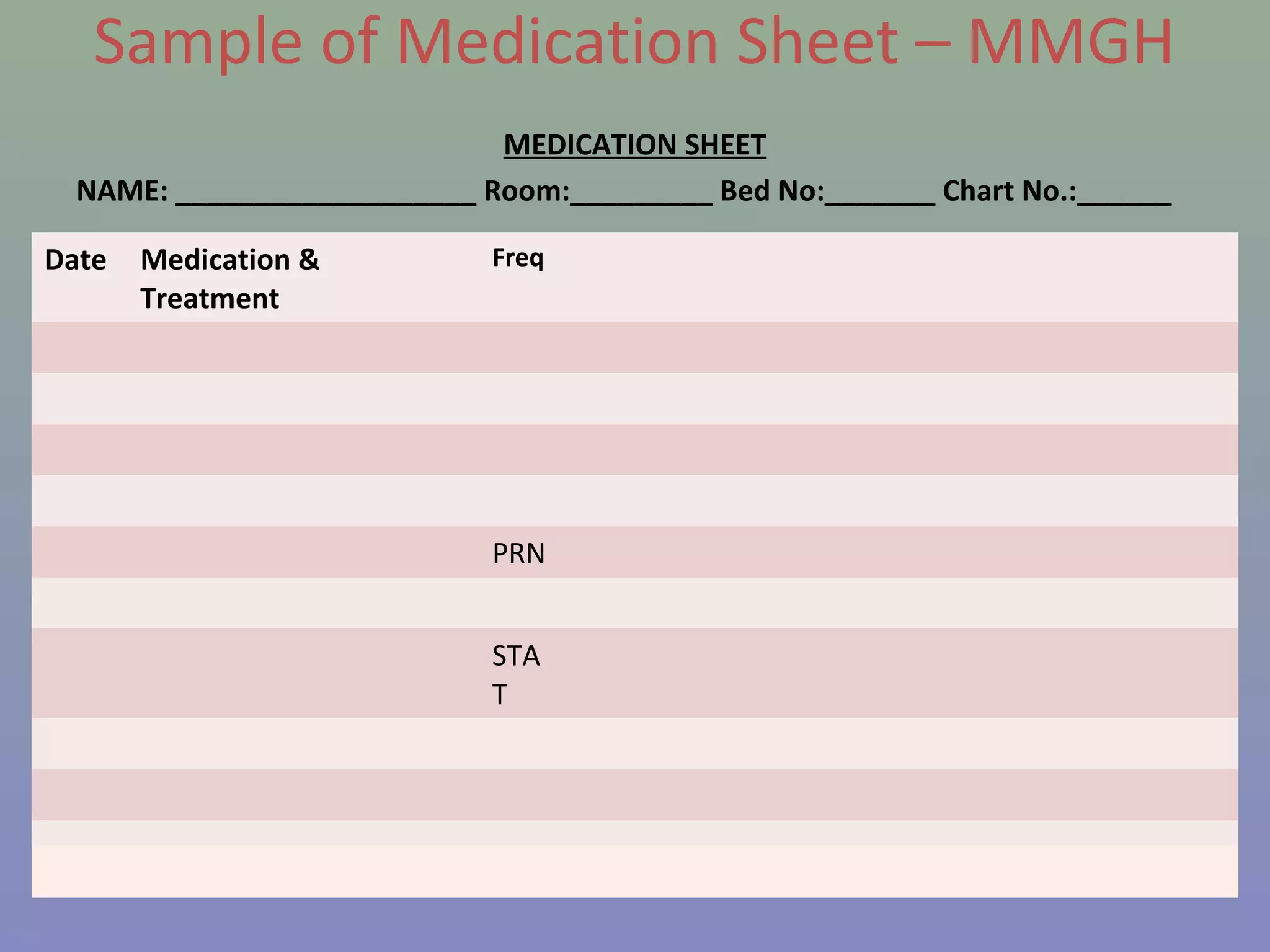
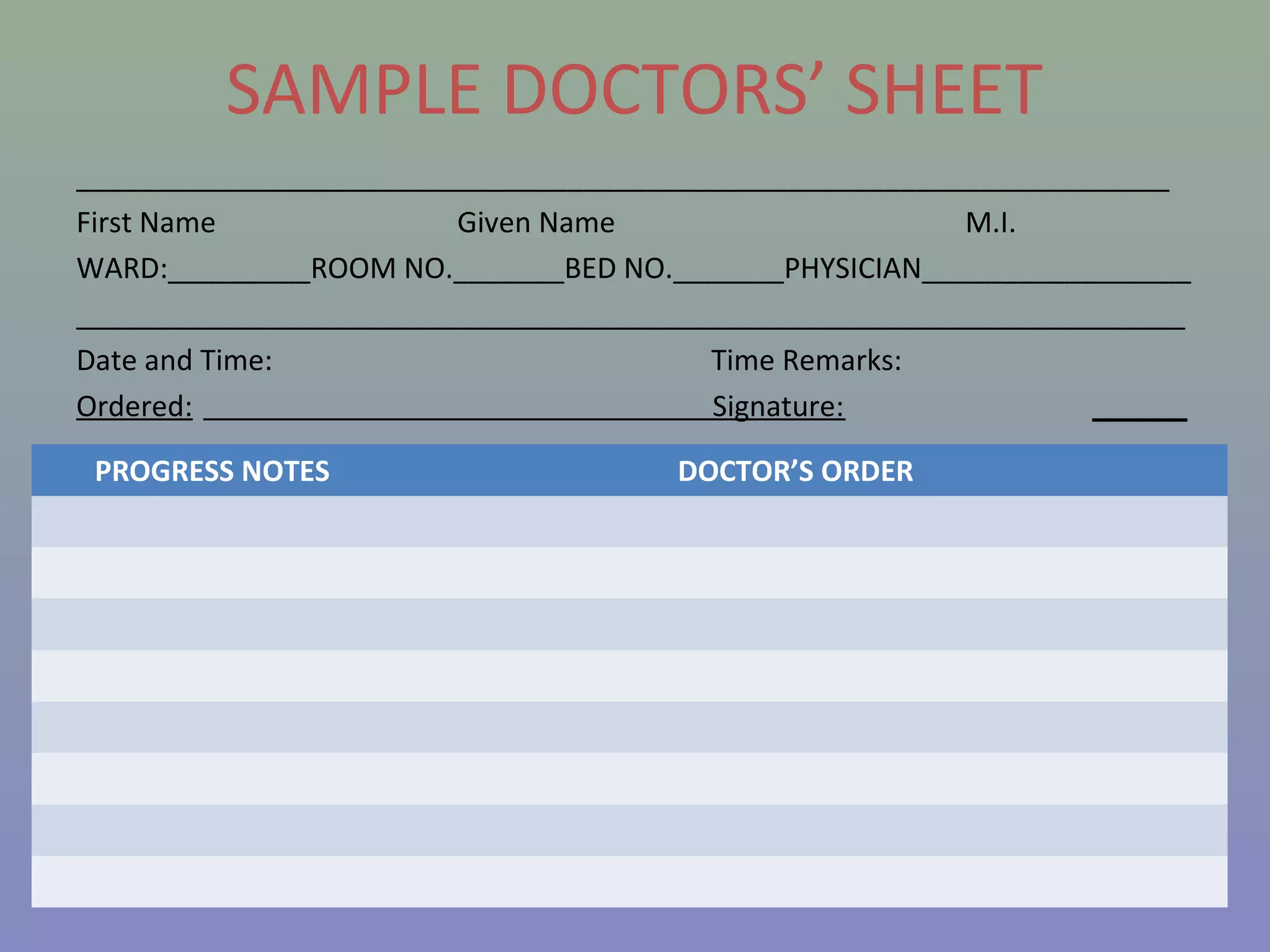
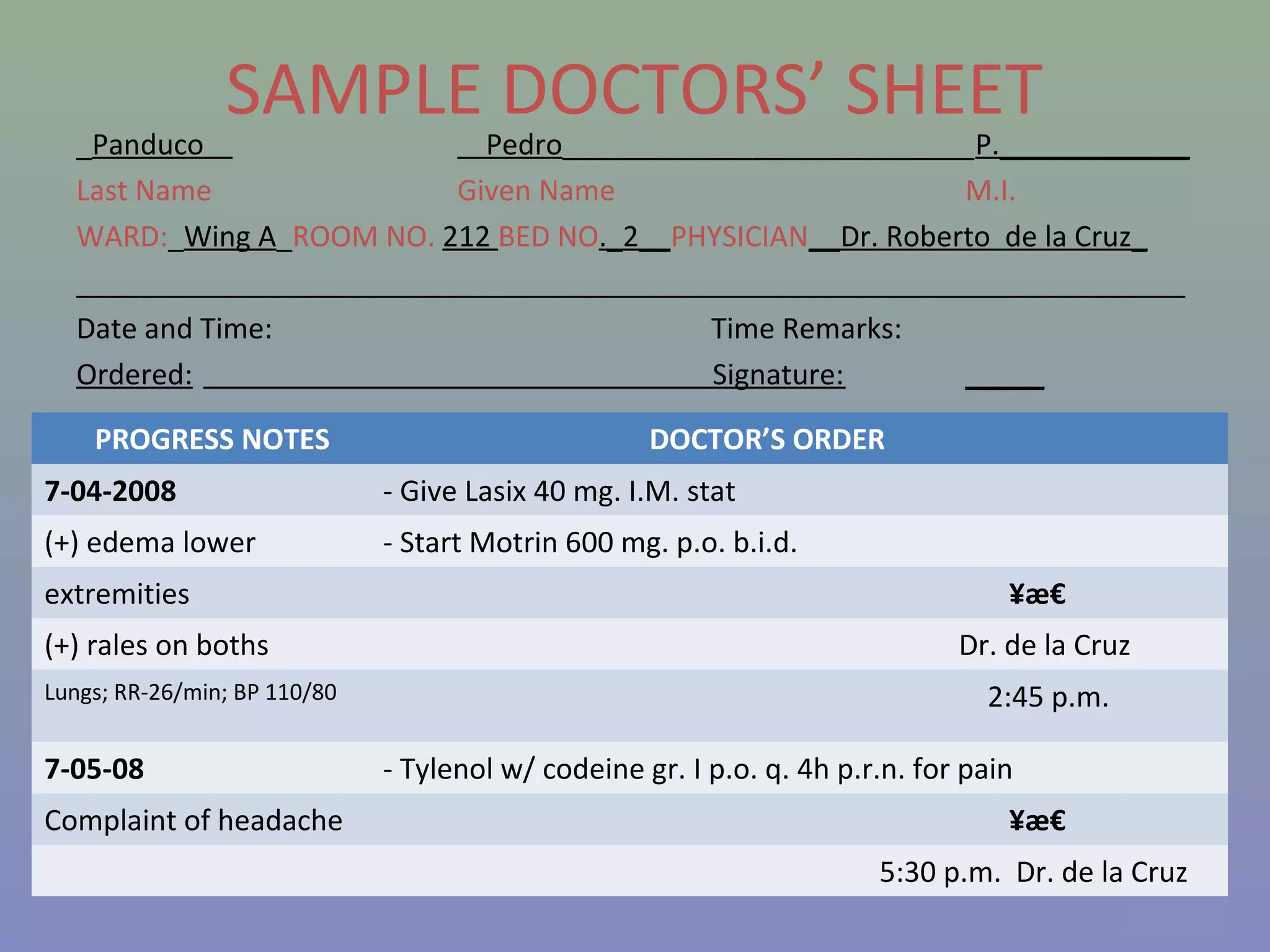
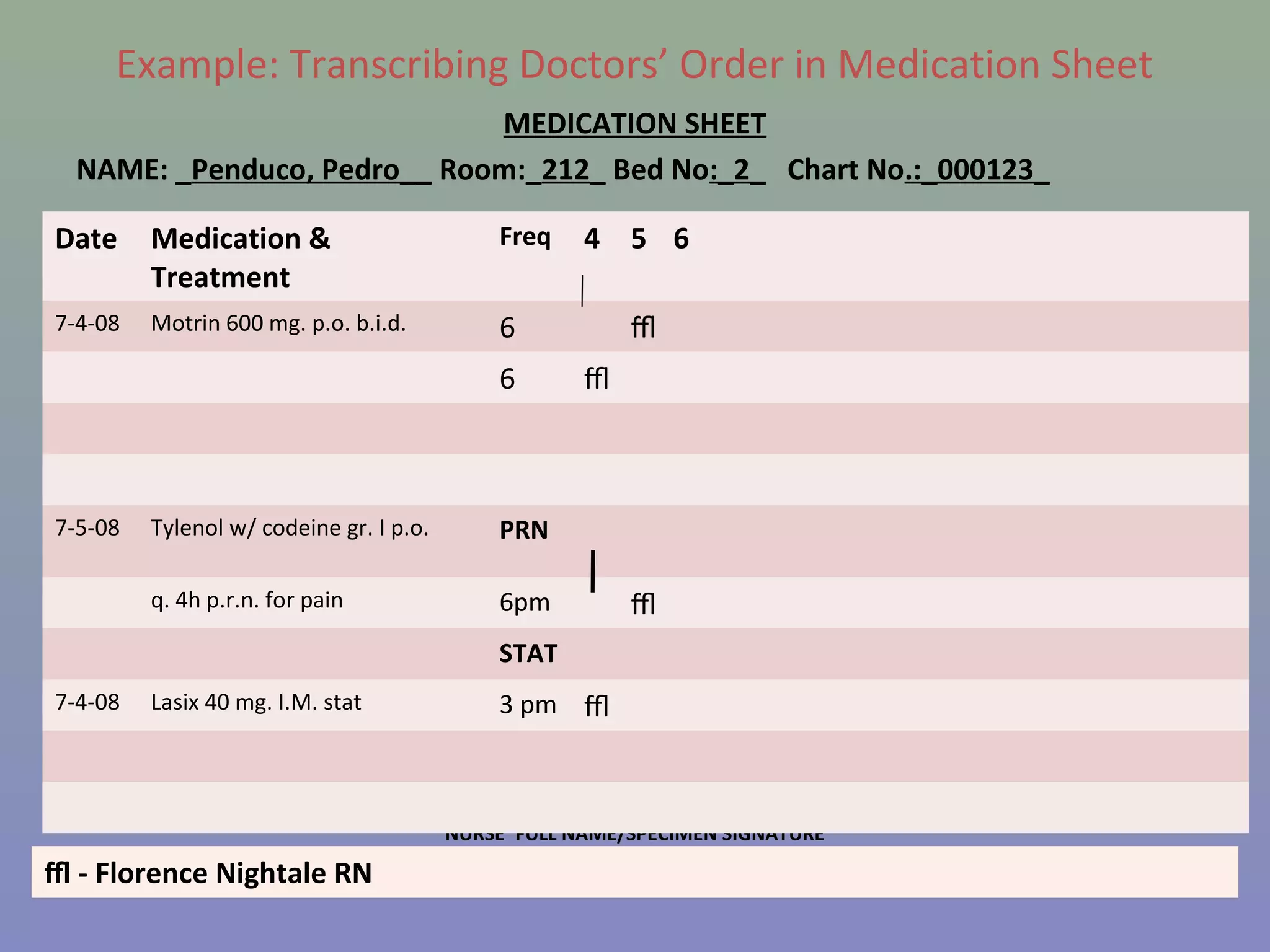

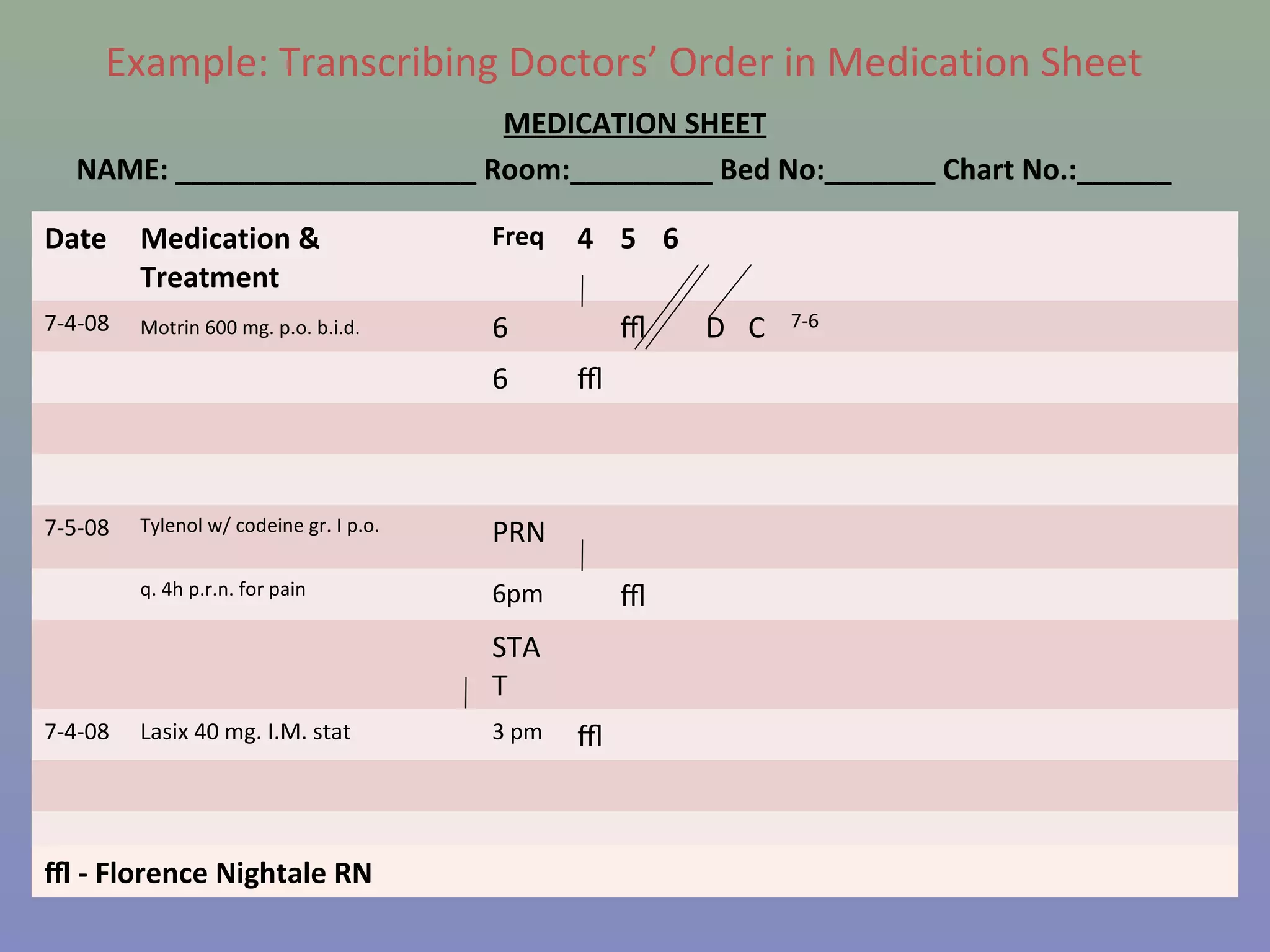

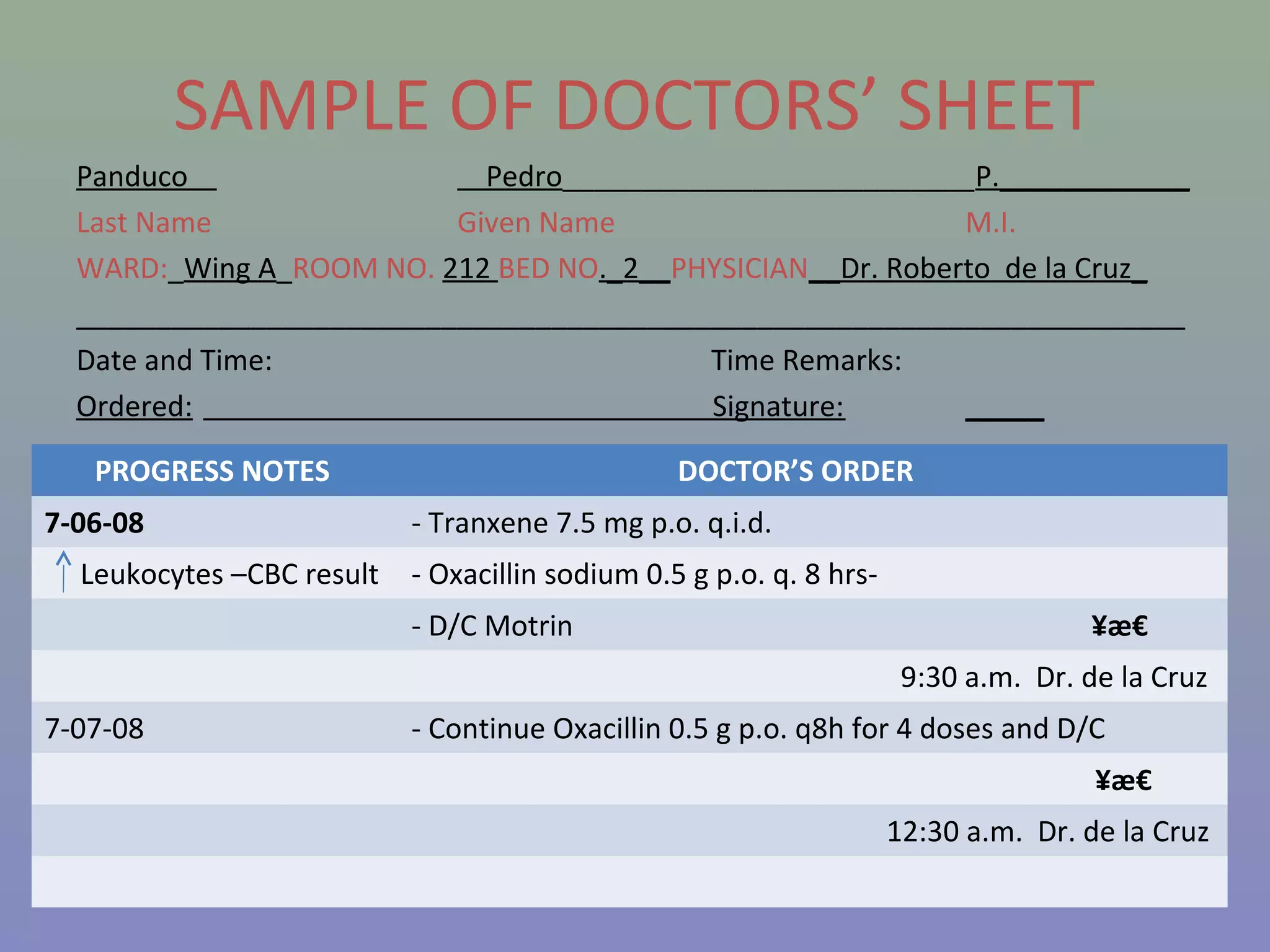
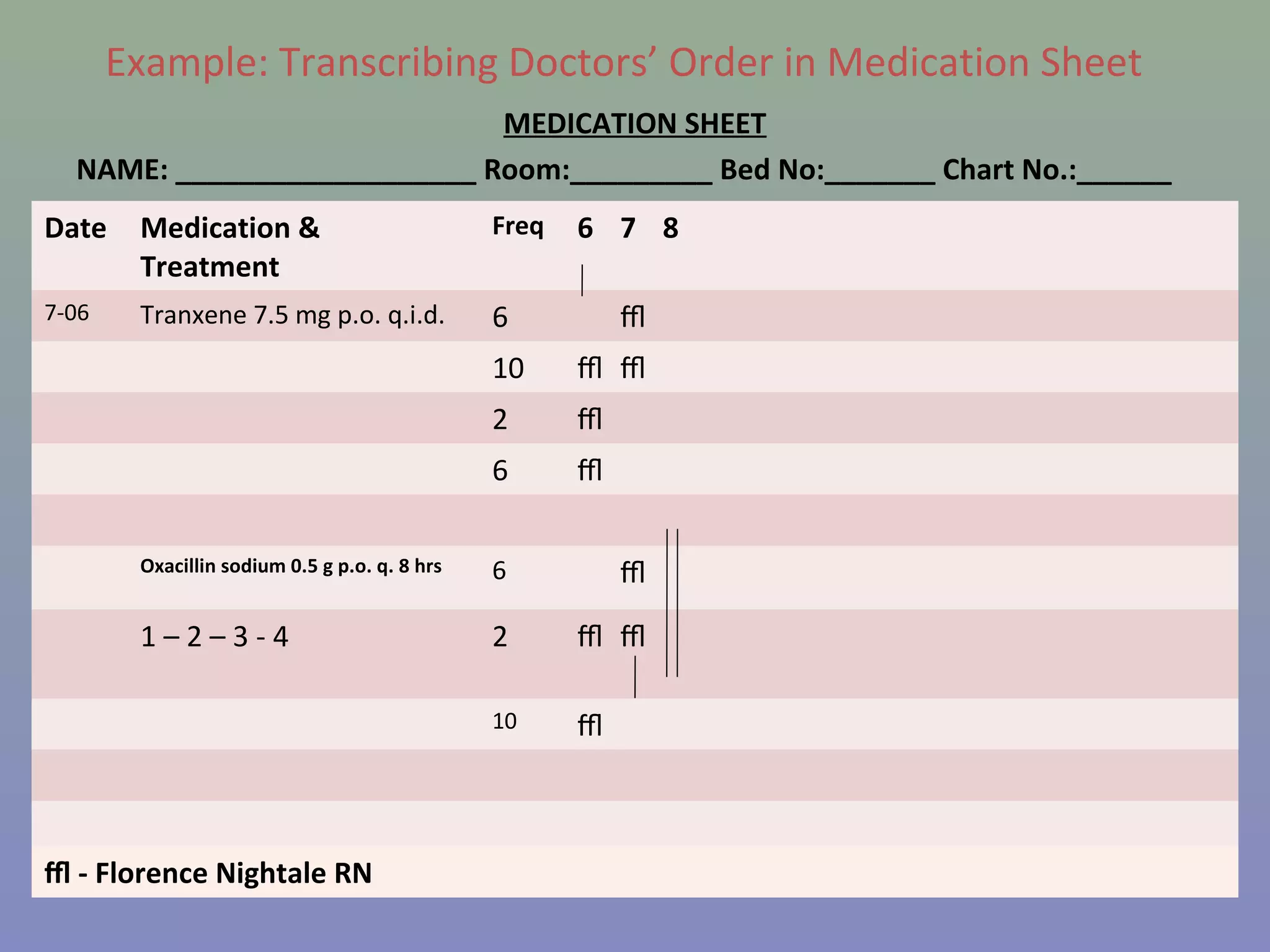
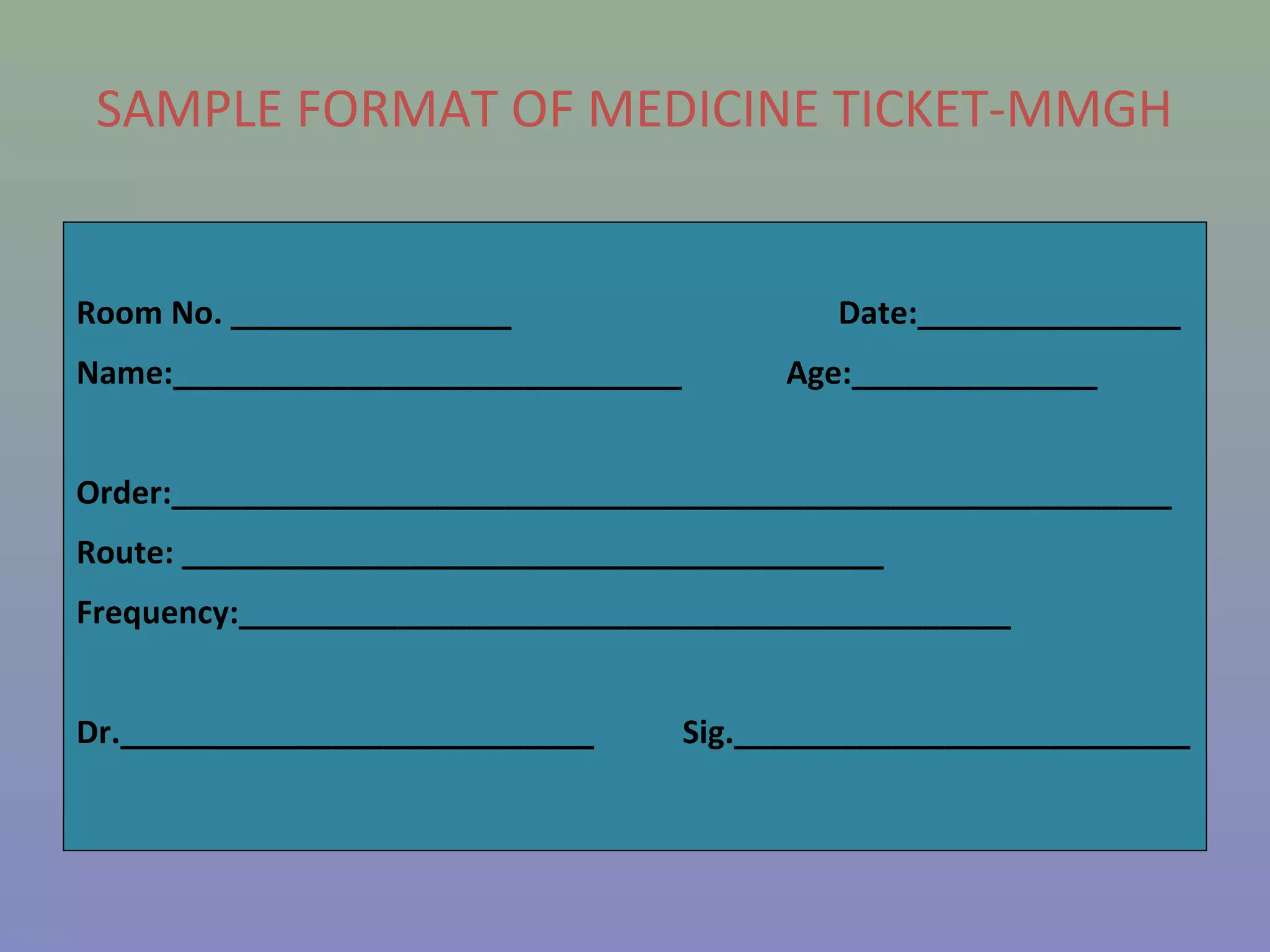

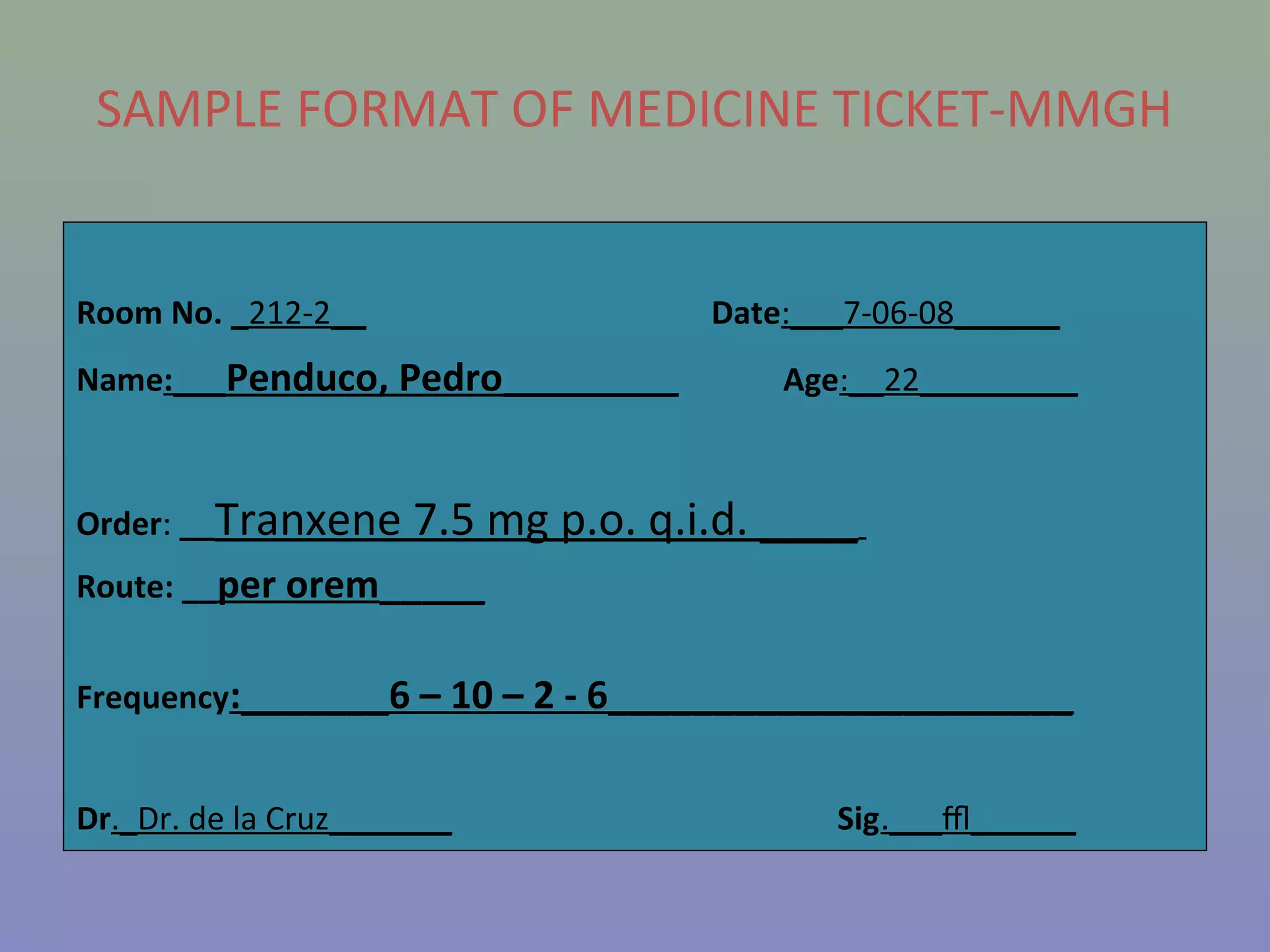
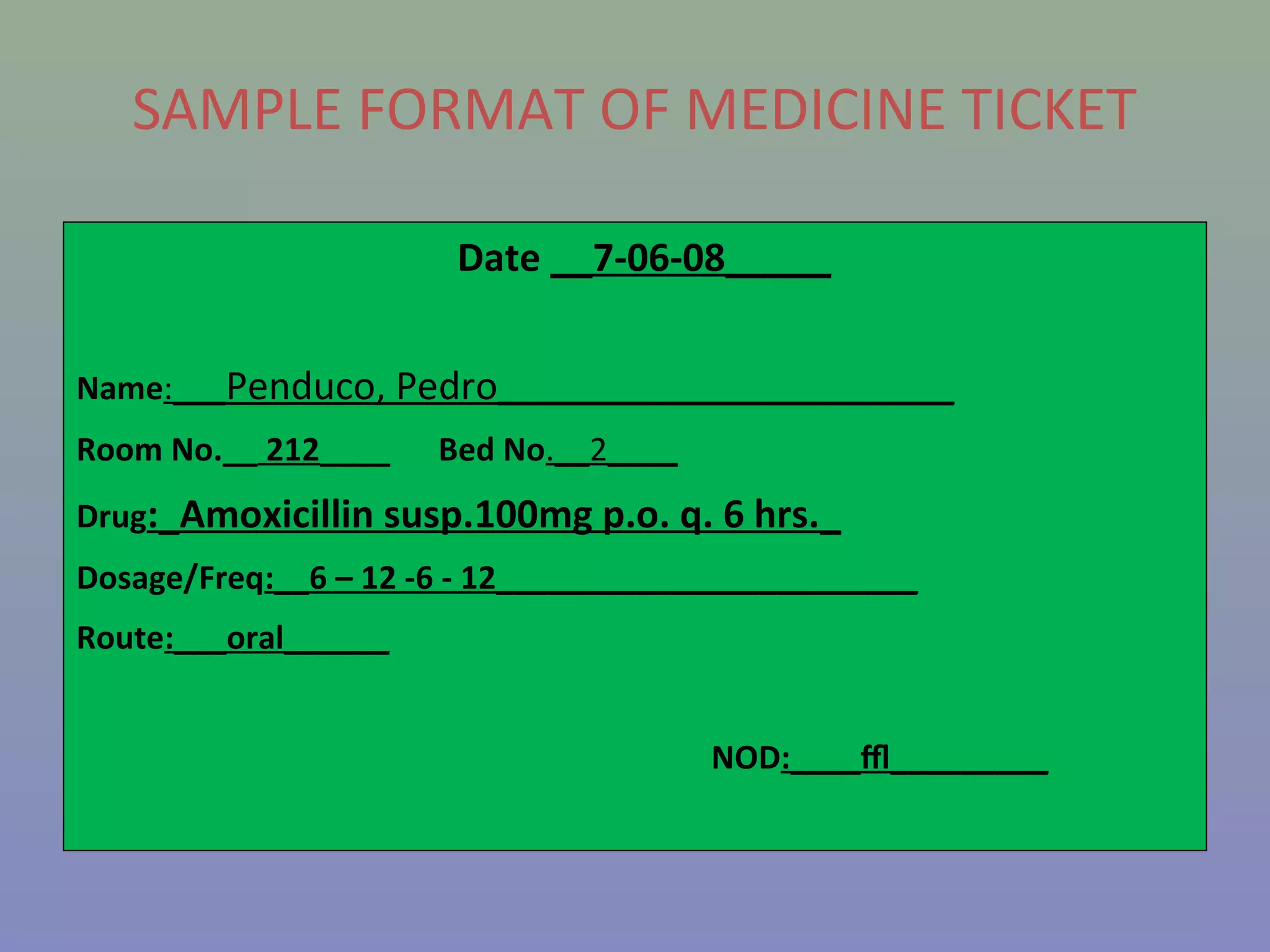

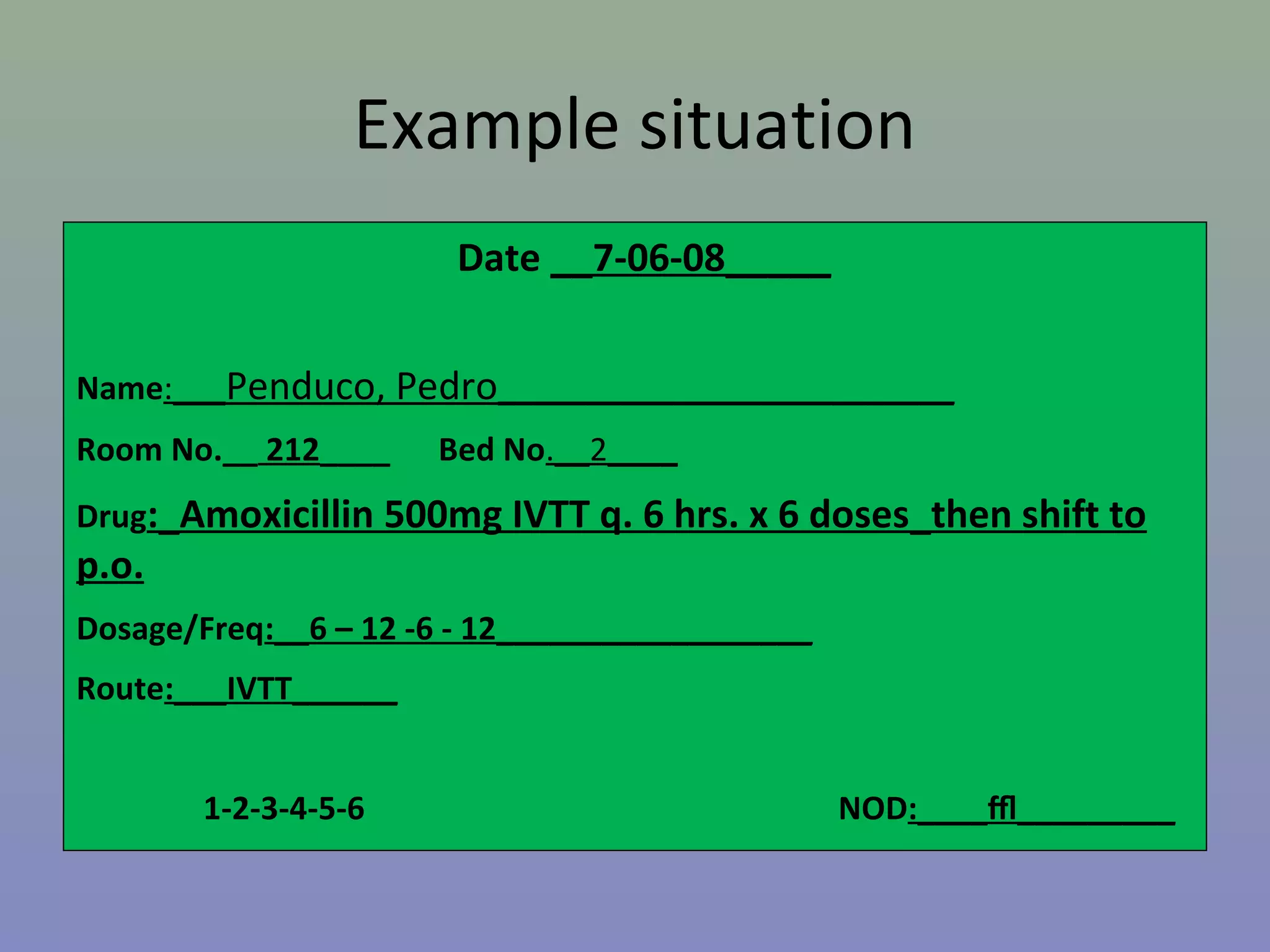

The document provides instructions for nurses on transcribing doctors' orders accurately. It discusses interpreting drug orders, using color coding and sample medicine tickets to organize medications by frequency. Common errors like misinterpreting times or dosages are outlined. Keys to accurate transcription include never altering original orders, writing legibly, creating new tickets for new orders, clarifying uncertainties, and signing sheets only after administering medications. Proper transcription is important to ensure patients receive the correct treatments.

































































![NANIME Medication Incidents and safe prescribing FY2 [part 2] 2016](https://cdn.slidesharecdn.com/ss_thumbnails/41fe4c34-641d-4dde-903d-e5c2ed417d3a-160603181352-thumbnail.jpg?width=640&height=640&fit=bounds)








































