

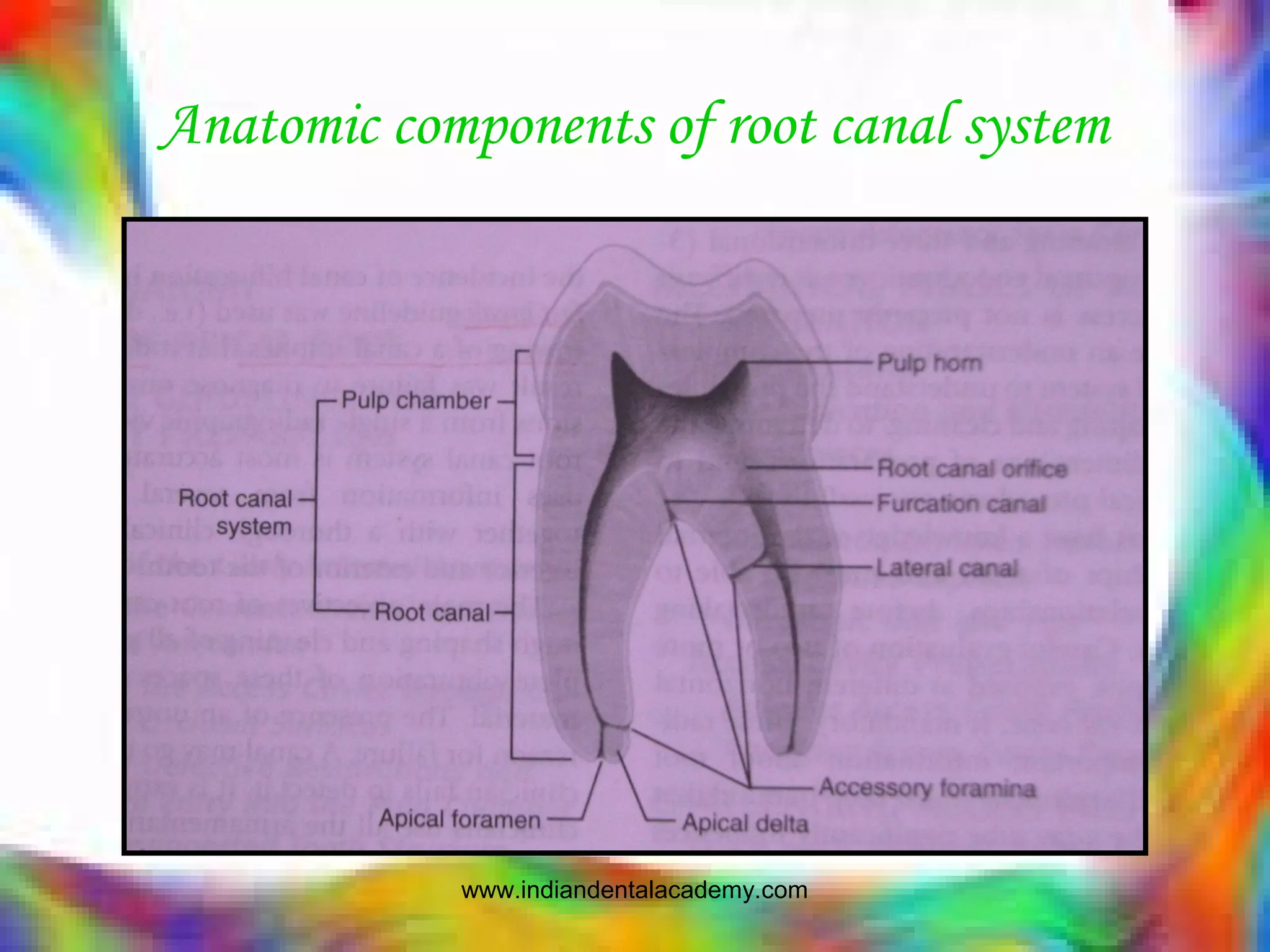
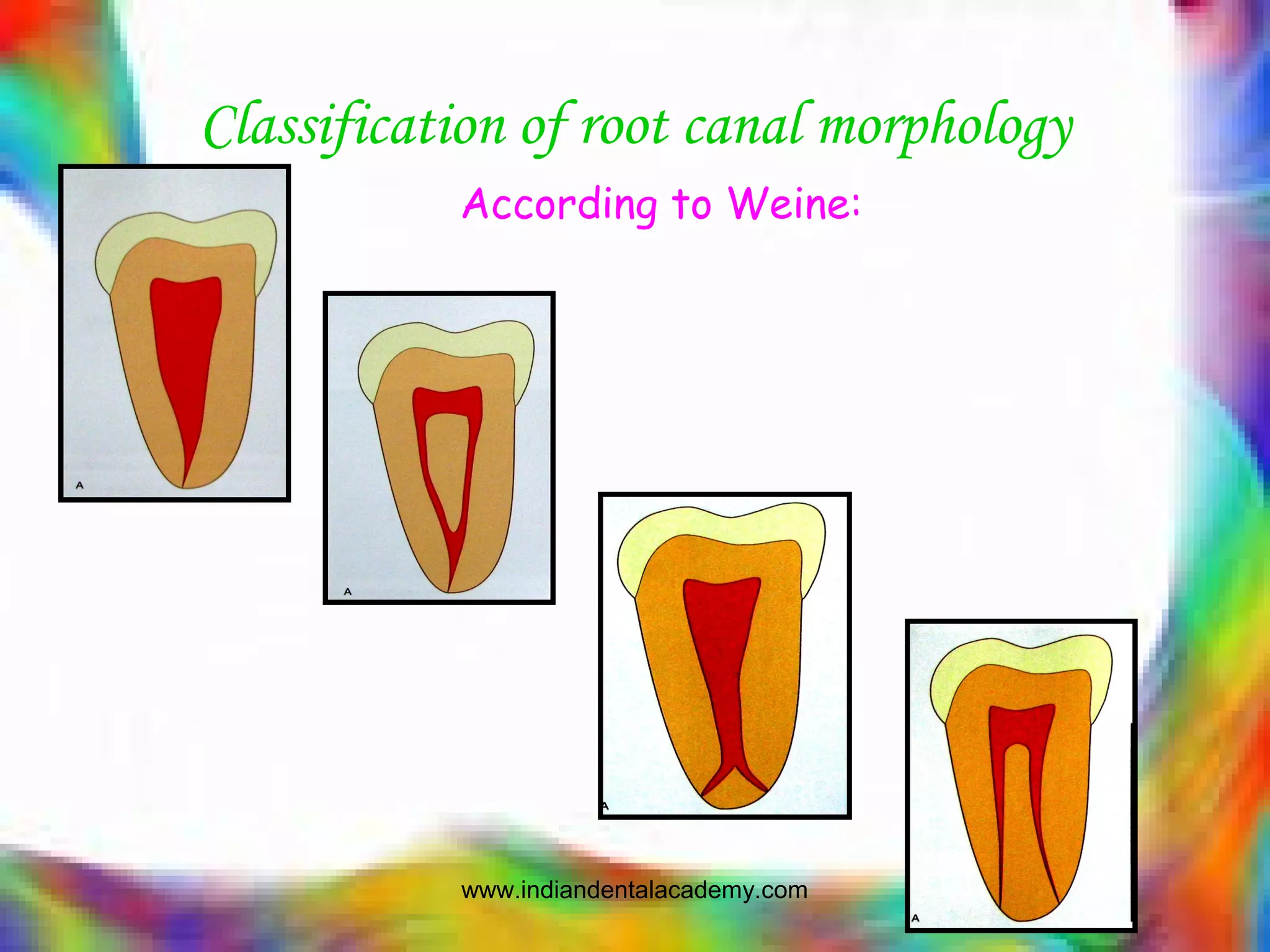

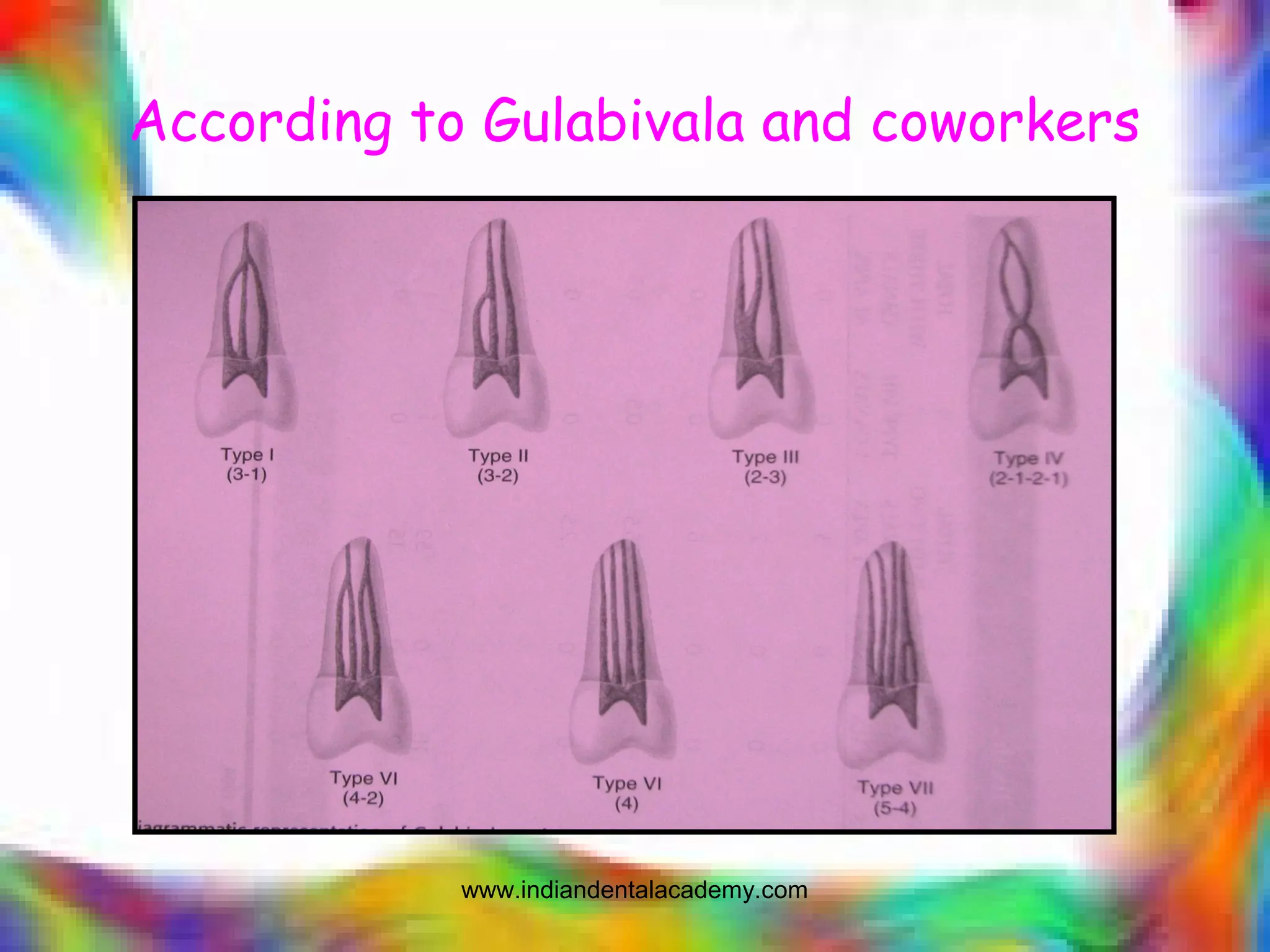
































This document discusses the anatomic conditions and morphologic variations of root canal systems and their impact on endodontic treatment success. It describes the components of root canal anatomy including the pulp chamber, root canal orifice, apical anatomy, accessory canals, buccolingual width and curvature. It also discusses classifications of root canal morphology and general considerations for treatment. Specific anatomic features like C-shaped canals, developmental anomalies and blunder buss canals are examined. The document emphasizes the importance of understanding root canal anatomy to optimize instrumentation and obturation.























































































