
Recommended
More Related Content
Similar to TMJ - Copy.pptx ANATOMY EXAMINITION DISORDER
Similar to TMJ - Copy.pptx ANATOMY EXAMINITION DISORDER (20)
Recently uploaded
Recently uploaded (20)
TMJ - Copy.pptx ANATOMY EXAMINITION DISORDER
- 2. • A joint is a point where two or more bones meet. There are three main types of joints; Fibrous (immovable), Cartilaginous (partially moveable) and the Synovial(freely moveable) joint. • Temporomandibular joint is the articulation between the temporal bone and the mandible. • It is a bilateral ginglymoid joint
- 3. DEVELOPMENT OF TMJ • Van der Linden et al. (1987)-the critical period of TMJ morphogenesis between weeks 7 and 11 of IU development. • Morimoto et al. (1987) describes a number of phases in TMJ development. STAGE DEVELOPMENT 7th week IU Meckel’s Cartilage extends from the chin to the base of the skull Appearance stage 8–9 IU) glenoid and condylar blastemata Preliminary stage 10–17 IU) articular disc, joint cavities, and condyle shows cartilage and endochondral ossification Completion stage (week 21 to term) all articular elements undergo growth and hematopoiesis begins 31st week IU Meckel’s cartilage transformed to anterior ligament of malleus and sphenomandibular ligament.
- 4. AGE DEVELOPMENT Birth Mandibular fossa- flat. Joint same level of occlusal plane 2 ½ - 6 years Mandibular fossa – deepens. Articular eminence increases in size 7 years Articular tubercle begins to become prominent 12 years. Articular layer- thickens cartilage layer -thins 20 to 25 years condyle contains cartilage , condyloid process and ramus lengthens
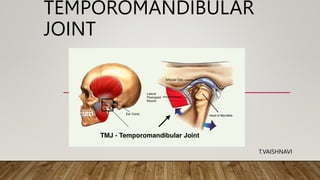
- 5. ANATOMY • TMJ is formed by the mandibular condyle and the mandibular fossa of the temporal bone. The articular disc separates these two bones from direct articulation . • The main components of TMJ • Mandibular condyles • Articular surface of temporal bone • Articular disc • Ligaments
- 6. • MANDIBULAR CONDYLE • The condyle is the part of mandible that articulates with the cranium, around which movements occur.It is roughly ovoid in shape when viewed from above . • TEMPORAL BONE • The condyle articulates at the base of the cranium with the squamous portion of the temporal bone. This portion of the bone is made up of , a concave mandibular fossa , in which condyle is situated and is called articular or glenoid fossa. • There is a convex bony prominence called the articular eminence.
- 7. • ARTICULAR DISC: • The articular disk is a thin, oval, firm, fibrous plate, placed between the condyle of the mandible and the mandibular fossa and divides the joint into a upper compartment and a lower compartment. • FUNCTION: • prevents friction between articulating surfaces. Proprioceptive fibers in disc help to regulate movements. • Distributes weight across the TMJ by increasing the area of contact.
- 8. LIGAMENTS • A ligament is a structure that connects two bones . • TRUE LIGAMENT:: Fibrous capsule of the joint Temporomandibular ligament • ACCESSORY LIGAMENT:: Sphenomandibular ligament Stylomandibular ligament
- 9. FIBROUS CAPSULE • It is a thin inelastic fibrous connective tissue envelope that attaches to the margins of the articular surfaces. • It is attached superiorly to whole circumference of mandibular fossa inferiorly to neck of mandible. • It stabilizes the joint. • It acts to resist any medial , lateral or inferior forces that tend to dislocate the articular surfaces.
- 10. Lateral Temporomandibular Ligament: • Its Fibers Are Directed Downwards And Backwards. • Above :Articular Tubercle • Below : Posterolateral Aspect Of Neck Of Mandible. • It Strengthens The Lateral Part Of Capsular Ligament.
- 11. SPHENOMANDIBULAR LIGAMENT • morphologically, it is remnant of cephalic end of meckel’s cartilage is attached superiorly to: spine of sphenoid bone inferiorly to: lingula of mandibular foramen laterally related to: lateral pterygoid muscle, auriculotemporal nerve, maxillary artery. medially related to: chorda tympani nerve. • near its lower end it is pierced by: mylohyoid nerves and vessels STYLOMANDIBULAR LIGAMENT: • It is thickened part of deep cervical fascia. • Above: lateral surface of styloid process. • Below: angle and adjacent part of posterior part of ramus.
- 12. RELATIONS OF TEMPOROMANDIBULAR JOINT:
- 13. • BLOOD SUPPLY OF TMJ • Predominant is superficial temporal artery branch of of maxillary artery • Condyle receives its vascular supply through its marrow spaces by way of inferior alveolar artery . • NERVE SUPPLY OF TMJ: • the auriculotemporal and masseteric branches of mandibular branch of the trigeminal nerve • LYMPHATIC DRAINAGE • Preauricular Nodes ,Parotid Nodes ,Submandibular Nodes
- 14. MOVEMENTS Movement TMJ Protraction Articular disc glides forward over upper articular surface. retraction Articular disc glides backwards over upper articular surface. Slight opening Head of mandible moves undersurface of articular disk like hinge Wide opening Hinge like movement followed by gliding of disc and head of mandible Chewing Head of right side glides forward along with disc, head on left rotates on vertical axis
- 15. • Muscles involved in MOVEMENTS • 1. Depression Of Mandible • Lateral pterygoid • Digastric • Geniohyoid • 2. Elevation of Mandible • Temporalis • Masseter • Medial Pterygoids • 3. Protrusion of Mandible • Lateral Pterygoids • Medial Pterygoids • 4. Retraction of Mandible • Posterior fibers of Temporalis
- 16. AGE CHANGES OF THE TMJ: • CONDYLE: • Becomes more flattened • Fibrous capsule becomes thicker. • Osteoporosis of underlying bone. • Thinning or absence of cartilaginous zone. • ARTICULAR DISK: • Becomes thinner. • Shows hyalinization and chondroid changes. • BLOOD VESSELS AND NERVES: • Walls of blood vessels thickened. • These age changes lead to: • -Decrease in the synovial fluid formation • -Impairment of motion due to decrease in the disc and capsule extensibility • -Decrease the resilience during mastication due to chondroid changes into collagenous elements • -Dysfunction in older people
- 17. TMJ EXAMINATION • Examined both clinically and radiographically. • PALPATION OF TMJ is determined by digital palpation.. • CREPITATION This is a grating or scalping noise that occurs on jaw movements. may be an early sign of degenerative joint disease.
- 18. • AUSCULTATION OF THE TMJ can be examined with a stethoscope. Also the timing of clicking during opening and closure can be noted. • CLICKING It occurs due to the uncoordinated movement of condylar head and TMJ disc. Joint clicking is differentiated as: • Initial clicking: it is a sign of retruded condyle. • Intermediate clicking: it is a sign of uneven condyle surfaces and articular disc. • Terminal clicking: it is an effect of the condyle being moved too far anteriorly in relation to the disc on maximum jaw opening.
- 19. RADIOGRAPHICALLY INDICATION AREA OF JOINT SEEN TMJ pain dysfunction syndrome Lateral aspect of: Glenoid fossa Articular eminence Joint space Condylar head Internal derangement Range of movement in joints •TRANSCRANIAL VIEW INDICATION AREA OF JOINT SEEN Tmj pain dysfunction syndrome Lateral view: Condylar head & neck Articular surface Osteoarthritis & rheumatoid arthritis Pathology-condylar head-cyst & tumor Fracture of neck & condyle TRANSPHARYNGEAL VIEW
- 20. REVERSE TOWNES VIEW TRANSORBITAL VIEW
- 21. • TMJ ARTHROGRAPHY • Norgaard (1940) • Indications: • Position and function of disk -pain and dysfunction-long standing • History of locking-persistent • Perforations of the disk and retrodiskal tissue. • Therapeutic : • To delineate loose bodies in the joint spaces • Diagnostic aspiration of joint fluid. • Intraarticular injections of steroids • Contraindications: • Infections in the preauricular region. • Patients allergic to contrast media. • Patients with bleeding disorders and on anticoagulant therapy
- 22. TEMPOROMANDIBULAR JOINT DISORDERS TRAUMA • Dislocation, subluxation • Hemarthrosis • Intracapsular fracture, extracapsular fracture • DISC DISPLACEMENT • ARTHRITIS
- 23. • DEVELOPMENTAL • Bifid condyle • Condylar hypoplasia • Condylar hyperplasia • ANKYLOSIS • NEOPLASMS • Benign tumors: osteoma, osteochondroma • Malignant tumors: Chondrosarcoma, fibrosarcoma, synovial sarcoma.
- 24. DISLOCATION • If oral opening proceeds to its maximum capacity, the condylar heads move to the anterior slope of the articular eminences. • Excursion of the condylar heads beyond these limits is abnormal and termed as dislocation.
- 25. • The thumbs are placed on the occlusal surfaces of the lower molars and fingertips are placed below the chin. Operator has to exert full body pressure and give downward pressure on the posterior teeth to depress the jaw and at the same time the fingertips are placed below the chin to elevate it by giving upward pressure. • Chronic recurrent (habitual) subluxation: capsulorrhaphy, meniscectomy, eminectomy, creating of a mechanical obstacle.
- 26. ANKYLOSIS OF TMJ • Hypomobility to immobility of the joint can lead to inability to open the mouth from partial to complete. • . • The treatment of TMJ ankylosis is always surgical. Early surgical correction of the ankylosed joint is highly desirable • CONDYLECTOMY, GAP ARTHROPLASTY, INTERPOSITIONAL ARTHROPLASTY
- 27. MPDS(MYOFASCIAL PAIN DYSFUNCTION SYNDROME) • Pain or discomfort. Deviation and limitation of motion of the Jaw. Joint noises - grating, clicking etc. Tenderness to palpation of the muscles of mastication • patient counselling and assurance symptomatic pain relief Nsaids. Diazepam — 2.5 mg. for 10 days. • heat application: 15-20 mins - 4 times per day
- 28. • Tmj arthroscopy tmj arthrocentesis
- 29. • ASSOCIATION BETWEEN TMJ DISORDERS AND PERIODONTIUM • American Dental Association states that after years parafunctional habit may trigger symptomatology and an occlusion dysfunction develops. • Interocclusal appliance therapy • Garib et al temporomandibular joint problems and periodontal condition in rheumatoid arthritis and concluded that patients with advanced RA are more likely to develop more significant periodontal and TMJ problems.
Editor's Notes
- .