Download as PDF, PPTX


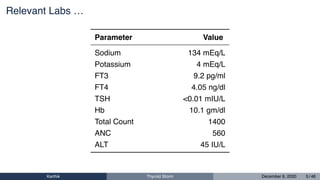
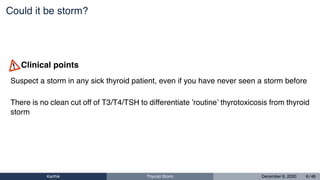


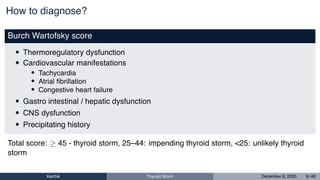
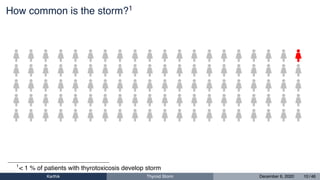






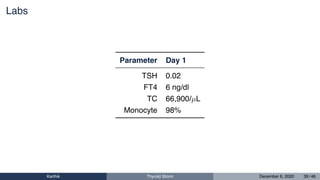
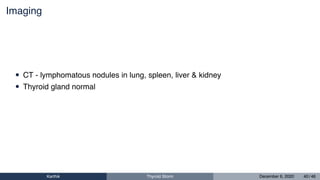
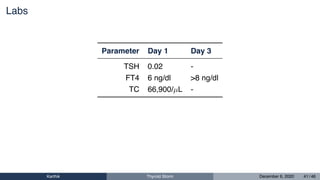
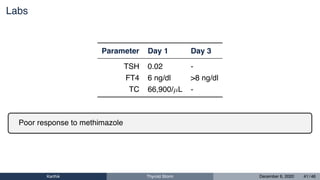

This document discusses the case of a 56-year-old woman who presented with fever, sore throat, and breathlessness and was diagnosed with thyroid storm. It provides details on her medical history, examination, labs, and treatment. The document also discusses two additional cases of thyroid storm and provides a summary of key points on diagnosing and treating thyroid storm.






















































































