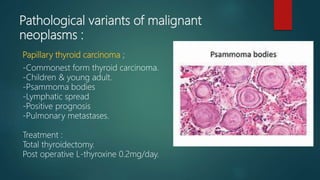
This document discusses thyroid neoplasms and solitary thyroid nodules. It notes that while thyroid cancer is rare, thyroid nodules are relatively common. For any solitary thyroid nodule, malignancy must be excluded through investigation like fine needle aspiration cytology. Less than 10% of solitary nodules are malignant, rising to 40% in patients with a history of neck irradiation. The document outlines the presentation, investigations, treatment approaches, and pathological variants of different types of thyroid cancer.