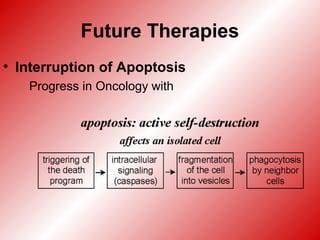
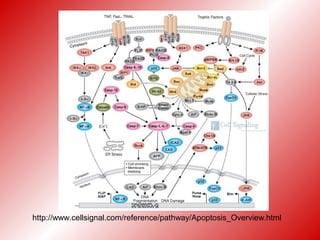
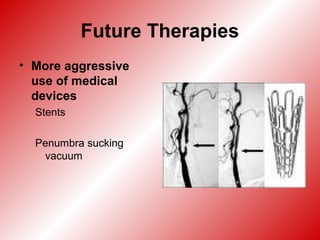
This document discusses the risks of hyperglycemia, hyperthermia, and hypoxia for stroke patients and provides strategies to mitigate these risks. It notes that hyperglycemia, hyperthermia, and hypoxia can all increase brain damage and worsen stroke outcomes. It recommends keeping patients normothermic, blood sugars between 80-140 mg/dL, and oxygen saturation levels normal to prevent additional brain injury. Future therapies discussed include hypothermia, medications to interrupt apoptosis and control edema, and more aggressive use of medical devices.

























































![Management of acute ischemic stroke including tia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofacuteischemicstrokeincludingtiaautosaved-180808183403-thumbnail.jpg?width=640&height=640&fit=bounds)








