The document discusses the evolution and effectiveness of intracorneal segments (ICS) for treating keratoconus and other ectatic conditions, noting initial uses for mild myopia. It summarizes various studies highlighting improvements in uncorrected and best-corrected visual acuity, as well as reductions in spherical equivalent and topographic values. Concerns about variable results, safety issues, and the need for better understanding and refinement of procedures and nomograms are also addressed.
![1st Author
(year)
Eyes (n) INTACS
Segments
Incision
(technique)
Follow-up
mean
(range)
Refractive change (D =
mean reduction) (± =
Visual change (m=
mean improvement) Published series
(thickness in mm) st. deviation)
Colin 10 As (0.45 inf +0.25 sup) Temporal 12 m (all) DK1=4.6D; DK2=3.6D Dcyl=2.70D (- UCVA m=3L BSCVA Follow-
(2001) 4.00-1.30D) m=2L 1st Eyes Ferrara / Incision Refractive Visual
up
Siganos 19 (A) inferior cone S (2x 0.45) (A)Temporal (sup-inf 11.3 m
impl.) (B) Superior (nas- 24 m)
(1- DK= 1.94 ±3.51D UCVA m=2.5L AVCC Author (n) Keraring (techniqu change (D = change (m=
(2003) 14 (B) central cone (50.8647.63D) m=1.7L (impr. 76% m=1 to mean
temp imp.)
DSE= 1.82 ±3.03D 6L; 12% worse, high Ks) (year) Segments e) mean reduction) mean
(range
Boxer Wachler 74 As (0.30-0.35 inf +0.25 Eje + Cyl (exc. if topo 9 m (1- DI-S: 25.626.60D UCVA m=4L BSCVA m=2L (thickness improvement)
(2003) sup) axis @90º of Cyl) 20 m) DSE=2.43D (-3.89-1.46D) (12% worse) )
in mm)
Hellstedt (2005) 50 As (0.45 inf +0.25 sup) Temporal 6.3±3.2m DK1=4.2D; DK2=3.3D UCVA m=1.0±2.0L BSCVA
(1-12 m) SIA = 2.9 ±2.9D m=2.2±2.3L (10% worse) Siganos[2 26 S (2x160º; + Axis 6m DK = no data UCVA
DSE=2.72D(-2.12+0.66D) 2] (2002) Dcyl=2.22D (- m=1.3L(88.4%)
Levinger 58 S (2x 0.30-0.45); As (1x 0.45 Temporal (Sup if central 12 m DK1=3.44D; DK2=2.74D UCVA m=3L(81%≥2L)
0.15-0.35) (manual) (min.)
4.42-2.20) BSCVA m=2.3L
(2005) inf, only if inf cone & SE<-3.0) cone & SE > -3.75) (all) Dcyl=1.57D (-3.34-1.97D) BSCVA m=0L (20/32
DSE=2.84D (-3.88-1.04D) ±2.0L; 10% worse ≥2L)
DSE=5.80D (- (0.370.60)
6.91-1.11D) (2 explants)
Alió 9 (p-central cone) 4 As (0.45 inf +0.25 sup) Temporal (+ axis) 36 m (36- DK=3.13D @6m (1.69D BSCVA m=2L
(2006) (inferior cone) or (1x 0.45 inf) 48 m) regression @36m) (0.460.66; maintained
DSE=1.45D (-5.40-3.95D) DI- 636m)
S: 7.094.27D Miranda[2 36 S (2x160º; + Axis 6m DK1=9.6D UCVA m≥2L
Alió 20 (A) K≤53D As (0.45 inf +0.25 sup) Temporal (+ axis) 6m DK: (A)=4.30D; (B)=6.19D BSCVA: (A) m=3.8L (B) 3] (2003) (62.352.7D) (77.78%) BSCVA
(2006) 5 (B) K≥54D or (1x 0.45 inf) (all) DSE: (A)=2.81D; (B)=2.25D m= -1.2L (in 3 eyes, 1x
0.25-0.35) topograp (3- 12
DK2=7.5D m≥2L (80.56%)
(significant only in A) implant) hic m) (58.150.6D) (VA worse =
Colin 57 S (2x 0.40-0.45) As Temporal (0º - 6m DK = 4.3 ±2.8D Dcyl= UCVA m≥2L (78% ) BSCVA
(2006) (0.30-0.45 inf +0.25-0.40 sup) 180º) (1-12 m) 1.52 ±1.60D m=2 to 8L (62% ) (6% worse (manual) Dcyl: no data none, 5
≥2L)
DSE= 3.07 ±2.54D DSE=2.49D (- extrusions)
Ertan 118 S (2x 0.25-0.45?) As (0.45 inf Temporal (?) (FsL) 12 m DK=3.90D (51.5647.66D) UCVA m=2L (81.3% )
7.29-4.80D)
(2006) +0.25 sup, inferior cone) DSE=3.85D (-7.57-3.72D) BSCVA m=1.8L (impr. 73.7% ,
worse 9.3%)
Ibrahim 186 S or As (0.25 á + Cyl axis 5 years DK = 4.48D (52.5348.05D) UCVA m=85.2% BSCVA Kwitko 51 S (2x160º; + Axis 13±8. DK =5.69D UCVA m=86.4%
(2006) 0.45) m=87.9% (48.7643.17D) BSCVA m=86.4%
(2004) 0.20-0.30) (manual) 7m
Kanellopoulos 20 As (0.35-0.45 inf +0.25- Temporal (above 6m DK= 3.10D (49.4546.35D) UCVA m=6L Dcyl=1.66D (- (11.7% worse,
(2006) 0.40 sup) horizontal) (6 -12 m) Dcyl=2.54D (-3.75-1.21D) (20/15420/28) BSCVA
3.82-2.16D) 10 extrusions)
Dsph=2.23D(-3.38-1.15D) m=3.5L (20/3720/22)
DSE=3.69D(-5.33-1.64D) DSE=1.53D (-
Rabinowitz 10 (A) manual 20 S (2x 0.35, 15 eyes) As Temporal (?) (A) A: 12 m DK: (A)=2.52D; (B)=2.91D DSE: UCVA: (A) m=3.6L; (B) m=4.1L 6.08-4.55D)
(2006) (B) Lfs (1x 0.35, 4 eyes; 0.35 inf manual (B) FsL B: 6 m (A)=2.96D; (B)=3.98D (N.S.) BSCVA (A) m=1.6L; (B)
+0.25 sup, 1 eye, all FsL) m=3.9L (all n.s.)
Sharma 17 (1x) 20 (2x) (inf. As (1x: 0.25-0.35) ó (2x: + Cyl axis 3m DK1: (1x)=2.76D; (2x)=0.93D DK2: UCVA: (1x) m=9L; (2x)
(2006) cones, incl. post-LASIK 0.30-35 inf, 0.25-0.30 sup) (1 – 13 m) (1x)=0.92D; (2x)=0.13D SIA: m=2.5L BSCVA: (1x) Shabayek 21 S, As + Axis 3m DK1=3.37D; UCVA m=2.5L
ectasia) S (2x 0.35, 1 eye) (1x)=5.69D; (2x)=1.58D
m=2.5L (2x) m<1L DK2=1.21D BSCVA m=1.7L
DI-S: (1x)=9.51D; (2x)=4.22D DSE: (2007) (120º- (FsL) (1-6
(1x)=1.45D; (2x)=2.26D DK =2.24D (70%) (5%
Colin 100 S (2 x 0.40-0.45) Temporal 24 m DK= 3.3D (50.146.8D) UCVA: m=1 to ≥5L (80.5% 160º; m) (48.7946.54D) worse, 1 grade IV
(2007) Dcyl=1.31D (-4.62-3.31D) BSCVA: m=1 to ≥5L
DSE=3.13D (-6.93-3.80D) 68.3% 14.6% worse 1-4L)
0.15-0.35) Dcyl=2.68D (- cone, 1 explant)
Kymionis 11 (A) inferior cone S (2x 0.45) (A)Temporal (sup- 5 years (58- DK= 1.57D (49.59 45.20 @6m UCVA m=2.8L (0-9L)
4.83-2.15D)
(2007) 6 (B) central cone inf impl.) (B) 78 m) 48.02D@60m) BSCVA m=1.4L (0-8L) (6% DSE=2.37D (-
Superior (nas-temp (6m60m change not signific.) worse 3L, 1 eye) 6.33-3.96D)
impl) DK1-K2=0.98D (4.463.48D)
DSE=2.52D (-5.54-3.02D) DK1 =3.93D; DK2
Barraquer 165 S, As + Cyl/K1 6m UCVA m=2.0L
Zare (2007) 30 As (0.35-0.45 inf +0.25- Temporal 6m (all) DK =1.94D (49.8447.90D) UCVA m=3L BSCVA
(unpublished) =2.27D BSCVA m=1.0L
0.40 sup) Dcyl=0.75D (-4.65-3.90D) m=2L (90º-210º; axis (3-27
DSE=3.0D (-6.93-3.23D) Dcyl=2.48D (- (6% worse ≥2L,
Ertan (2008) 306 S (2x 0.25-0.45?) As Temporal (?) (FsL) 10.4 ±5m (4- DK =2.79D (50.7047.91D) UCVA m=2.5L(75.7%) 0.15-0.35) (manual, m) 5.91-3.43D)
(0.45 inf +0.25 sup, inf. 30 m) Dcyl=0.29D (-4.11-3.82D) BSCVA m=2L (71.6% ) (3.7% 5 extrusions)
cone) DSE=3.09D (-7.81-4.72D)
worse ≥2L) FsL) DSE=3.57D (-
Shetty (2008) 14 (stage III cone) S (11 eyes); As (3 eyes 0.45 K1 axis (Orbscan) 6m DK =3.59D (53.0149.42D) UCVA m=1.1L BSCVA 5.21-1.64D)
inf +sup “thinner” ¿?) (1-12 m) Dcyl=1.25D (-4.89-3.64D) m=1.7L (7.14% worse 1L)
DSE=4.20D (-9.13-4.93D)](https://image.slidesharecdn.com/barraquer-110507143614-phpapp01/85/The-SA-ANA-classification-3-320.jpg)
![ICS for KC: Results (summary)
summary)
All agree they are “Effective”, BUT…
“Effective”
►Increased UCVA ~ 2 - 3 lines (average)
►Increased BSCVA ~ 1 - 4 lines (~ 2 ave.)
ave.)
►Decreased Spher.Eq.
Spher.Eq. ~ 1.5 – 4.2 D (5.8 w KR)
►Decreased Topo. K
Topo. ~ 1.5 – 4.5 D (8.0 w KR);
►Decreased Refract. Cyl. ~ 0.3 – 2.7 D
Cyl.
[50-
[50-65% ave.: NOT a “REFRACTIVE” procedure]
ave.:](https://image.slidesharecdn.com/barraquer-110507143614-phpapp01/85/The-SA-ANA-classification-4-320.jpg)
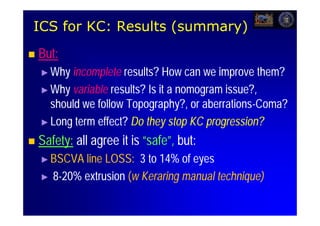



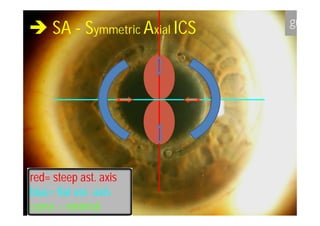
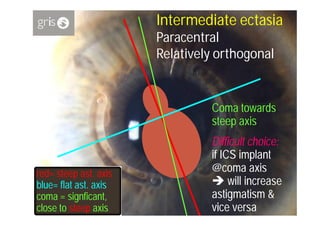
![Central, symmetric ectasia/conus
[ also: Regular astigmatism (congenital or post-PK);
Mild myopia (congenital or residual after Rx.)]
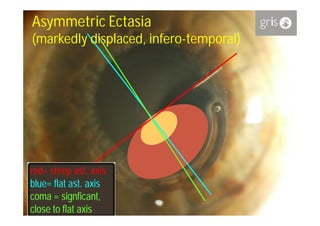
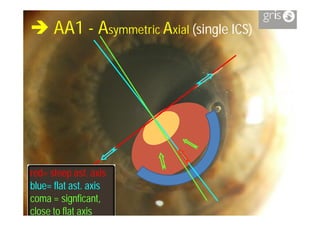
red= steep ast. axis
ast.
blue=
blue= flat ast. axis
ast.
coma = minimal](https://image.slidesharecdn.com/barraquer-110507143614-phpapp01/85/The-SA-ANA-classification-15-320.jpg)












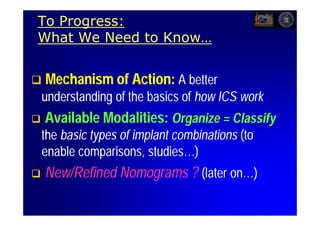
![Summary
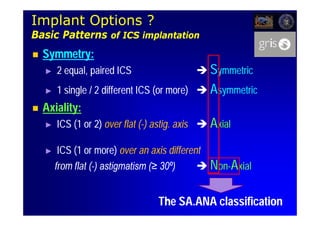
The availability of multiple ICS types demands a
classification to enable a meaningful comparison
between implant series.
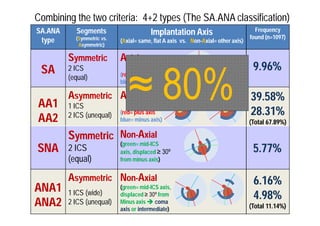
Observed ICS implantation modalities (n=1097) allow a simple
while comprehensive classification based on 2 criteria: symmetry
criteria:
& axiality. Combining the 2 criteria results in 4 types:
axiality.
The SA.ANA classification
SA = Symmetrical & Axial (always 2 equal ICS, @same, flat axis) = 9.96%
AA = Asymmetrical & Axial [either 1 (AA1) or 2 (AA2) ICS] = 67.89% (total)
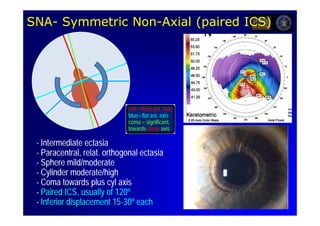
SNA = Symmetrical & Non-Axial (always 2 equal ICS, @different axis) = 5.77%
on-
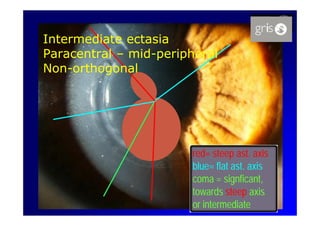
ANA = Asymmetrical & Non-Axial [either 1 (ANA1) or 2 (ANA2) ICS] = 11.14%
on-](https://image.slidesharecdn.com/barraquer-110507143614-phpapp01/85/The-SA-ANA-classification-34-320.jpg)












































































