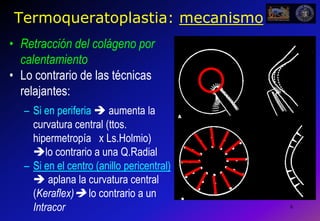
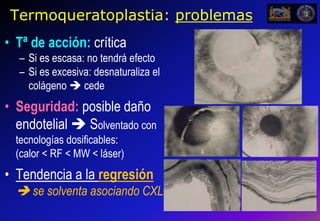
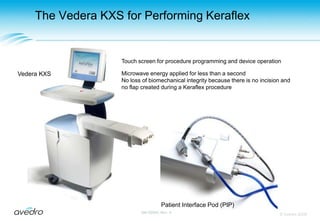
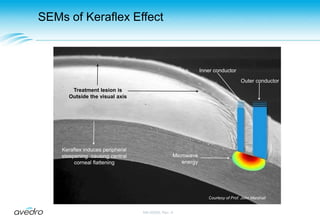
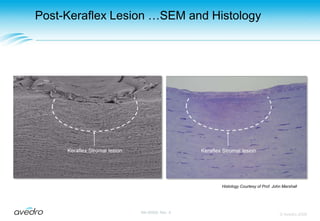
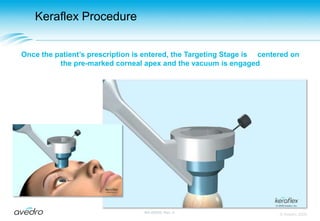
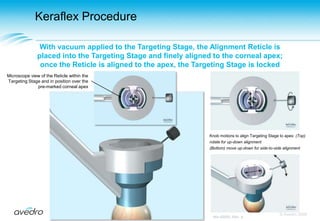
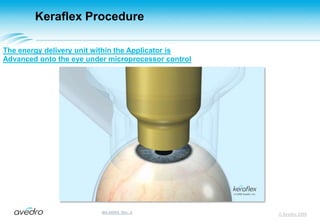
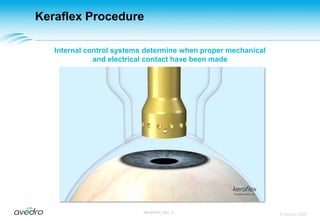
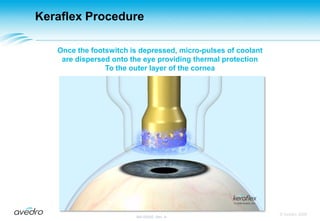
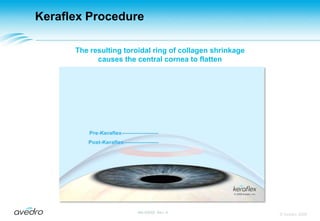
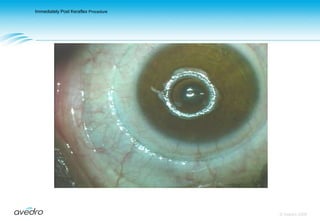
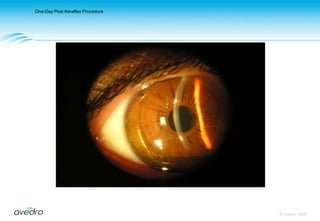
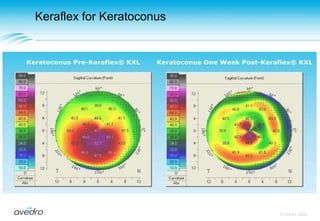
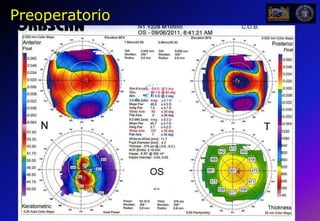
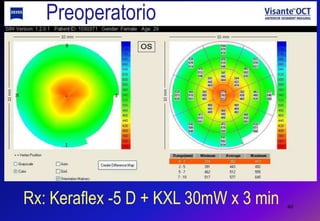
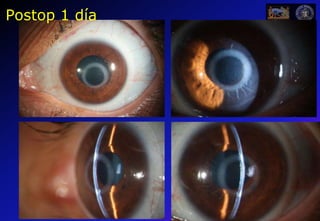
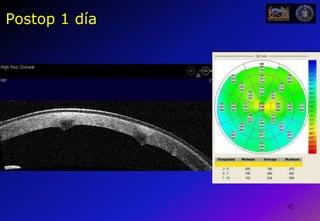
This document describes a new procedure called Keraflex, which combines corneal molding using microthermal keratoplasty and accelerated corneal collagen crosslinking. Keraflex uses microwave energy applied in a ring pattern to the peripheral cornea to induce central corneal flattening for the treatment of myopia and keratoconus. It is a minimally invasive procedure that does not require flap creation. The document provides details on the Keraflex procedure and equipment, as well as preclinical research demonstrating the biomechanical effects and safety profile of combining microthermal keratoplasty with accelerated crosslinking.