














![Systematic approach to EEG abnormalities
• The interpretation of EEG is associated with a poor inter-
oberserver reliability.
• Pattern recognition is inherently prone to pitfalls when rules
[of polarity] and convention are ignored.
• Problems of fluctuation in the accuracy of EEG interpretation
may vary from person to person and even in the same person
over time.
• There are guidelines available for conducting EEG studies, but
those available for defining and identifying EDs do not exist
for EEG interpretation.
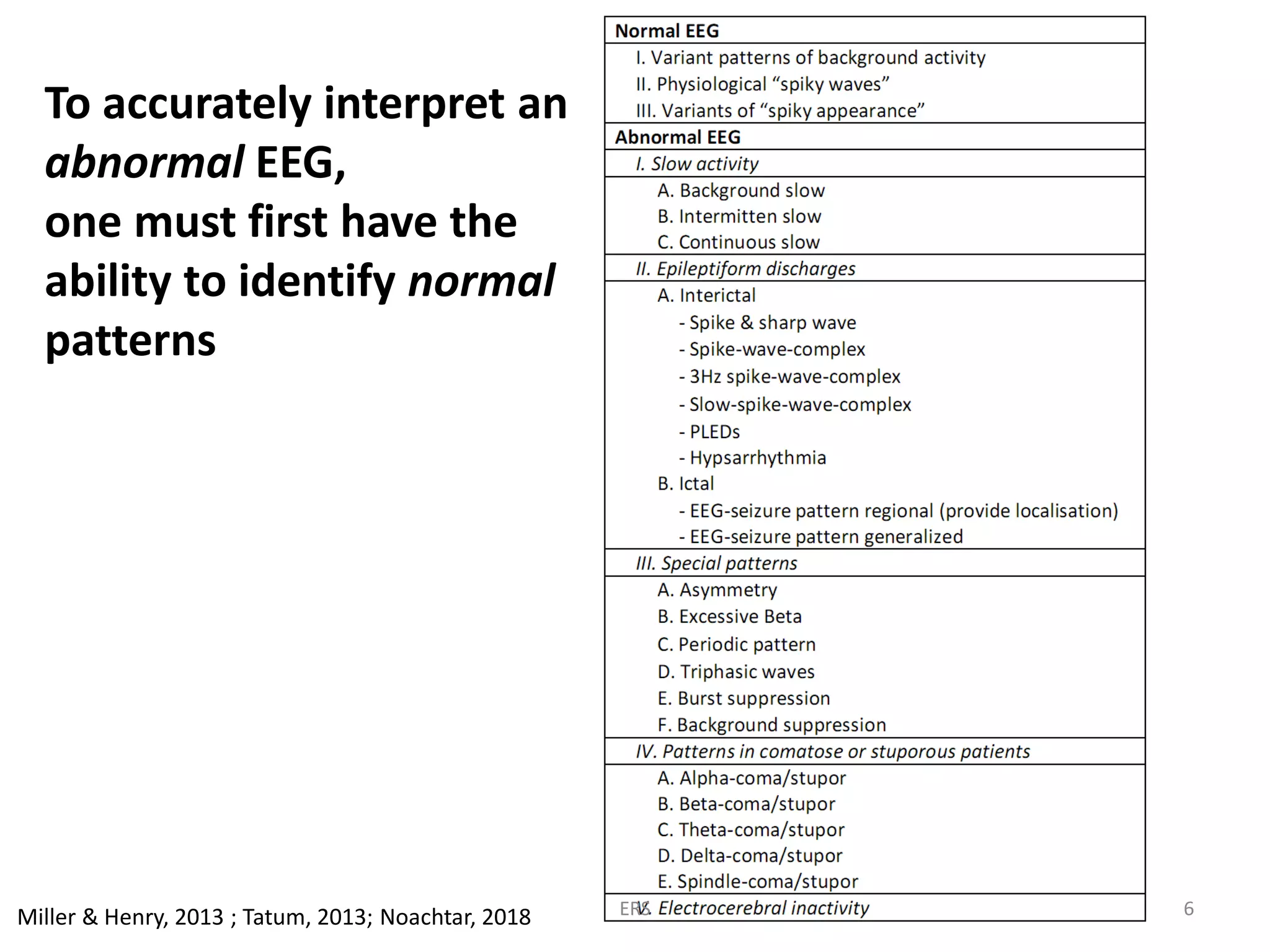
• It is important to follow a systematic approach to the
classification of EEG abnormalities.
Miller & Henry, 2013; Tatum, 2013; Noachtar, 2018 ERS 22](https://image.slidesharecdn.com/eeginterpretationphilosophy-ersifa-180826085131/75/The-Philosophy-of-EEG-Interpretation-22-2048.jpg)
![EEG interpretation & report [1]
• Requires knowledge of the patient’s age, past medical and
medication history, their clinical condition during the EEG,
particularly level of consciousness and responsiveness.
• Should follow a standard format that includes a factual
description, a classification and a clinical interpretation of the
EEG record.
• EEG interpretation summarizes the results of the EEG and
gives a clinical interpretation in light of the diagnosis and the
questions posed by the referring physician.
• Terminology of the EEG interpretation should follow common
neurological and clinical practice and use terms
understandable to other physicians not specialized in EEG
Noachtar, 2018 ERS 23](https://image.slidesharecdn.com/eeginterpretationphilosophy-ersifa-180826085131/75/The-Philosophy-of-EEG-Interpretation-23-2048.jpg)
![EEG interpretation & report [2]
• All EEG phenomena should be described as precisely as
possible in terms of frequency, amplitude, phase relation,
waveform, localization, quantity, and variability of these
parameters.
• The terminology used should follow international standards
and recommendations
Noachtar, 2018 ERS 24](https://image.slidesharecdn.com/eeginterpretationphilosophy-ersifa-180826085131/75/The-Philosophy-of-EEG-Interpretation-24-2048.jpg)


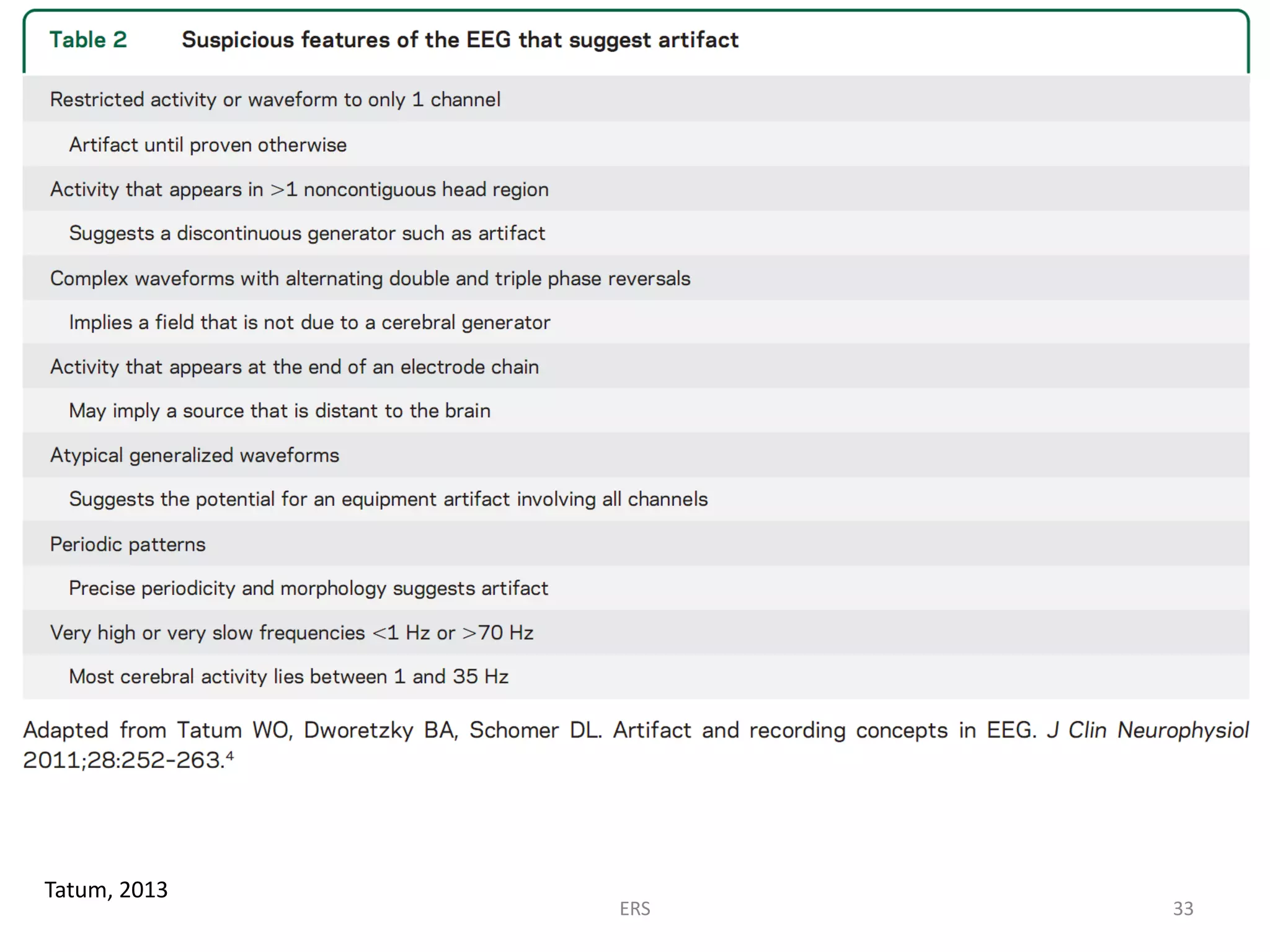
![• The diagnosis of seizures relies mainly on a good history,
which requires skills and time.
• The importance of the EEG is [often] overemphasized, and it is
especially detrimental when it is interpreted out of clinical
context.
• Overreading is more harmful than underreading.
• Every EEG should be interpreted with care and caution to
avoid pitfalls.
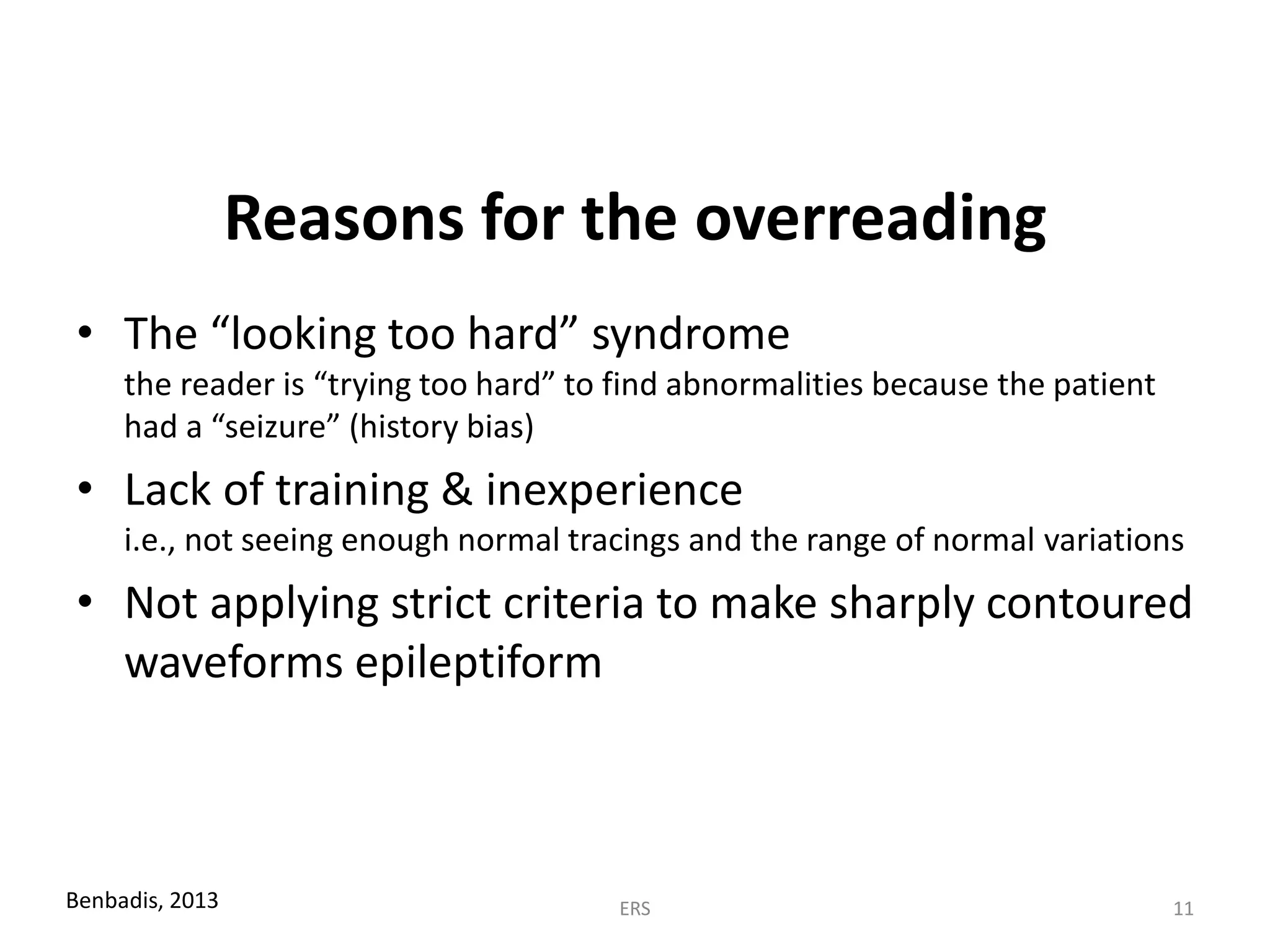
• Proper training is a crucial aspect of minimizing as many of
the errors as possible.
ERS 28](https://image.slidesharecdn.com/eeginterpretationphilosophy-ersifa-180826085131/75/The-Philosophy-of-EEG-Interpretation-28-2048.jpg)

















The document discusses the complexities and potential pitfalls of EEG interpretation in diagnosing epilepsy, highlighting that many misdiagnoses stem from overinterpreting normal EEG findings. It emphasizes the importance of accurate training and cautious analysis to avoid false-positive results that can lead to inappropriate treatments. The key takeaway is that while EEGs are important, their findings must always be contextualized with the patient's clinical history and symptoms, as a normal EEG does not rule out epilepsy.




























![EEG & Epilepsy syndromes report [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/e189c60d-77a3-4067-bdbe-fe484f4e5901-150602002311-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

























































