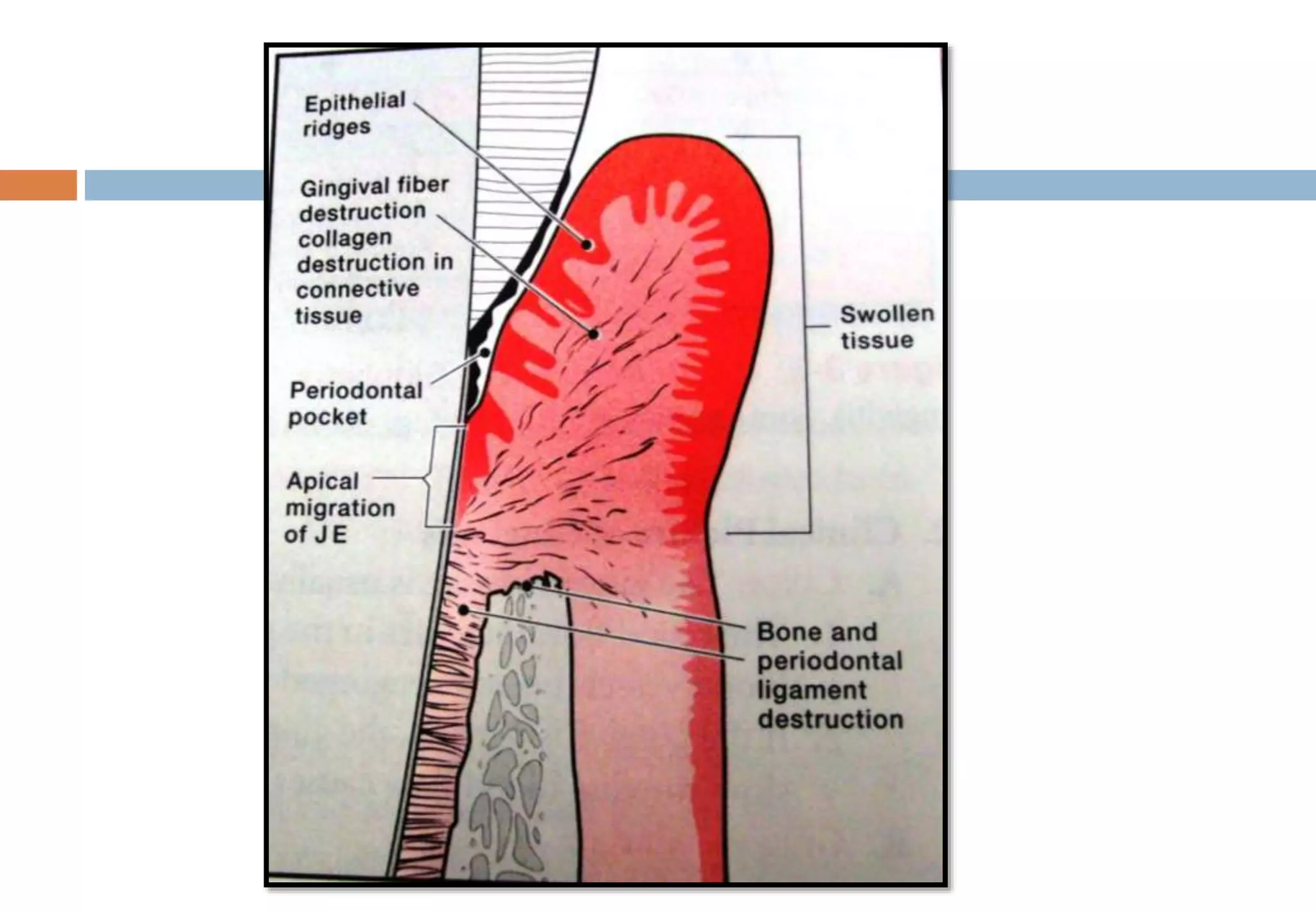
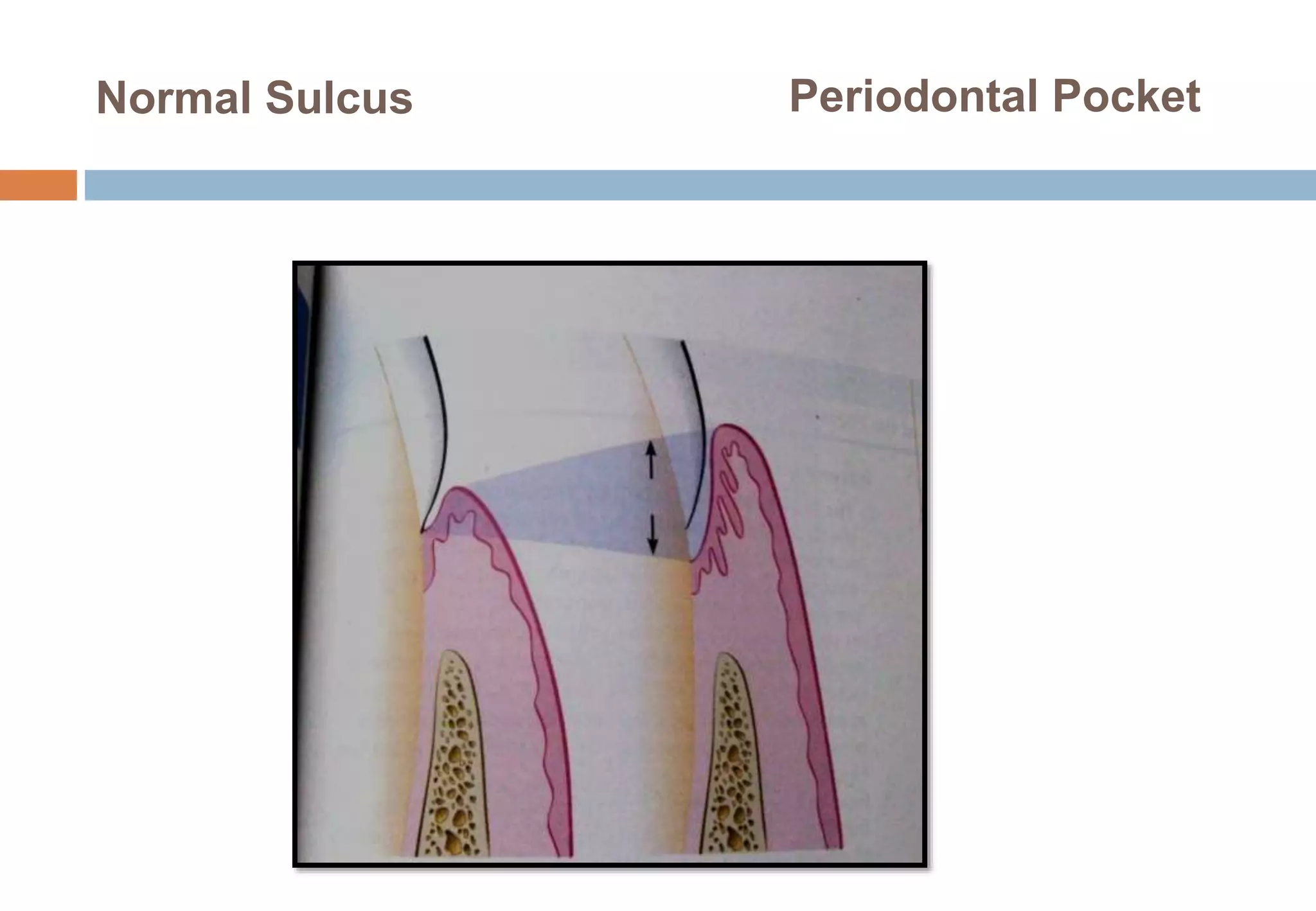
This document summarizes the key features and pathogenesis of periodontal pockets. It defines a periodontal pocket as a pathologically deepened gingival sulcus with loss of connective tissue attachment and bone. Pockets can be classified based on their location relative to the alveolar bone or the involved tooth surfaces. The formation of pockets starts with bacterial challenge causing gingival inflammation and destruction of connective tissue fibers. Over time, the junctional epithelium migrates apically, forming the periodontal pocket. The pocket walls undergo degenerative changes with bacterial invasion and host inflammatory response. Treatment involves scaling and root planing to remove bacterial deposits and necrotic cementum.