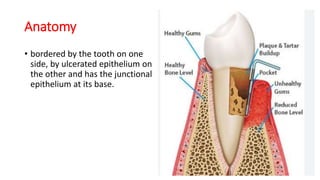
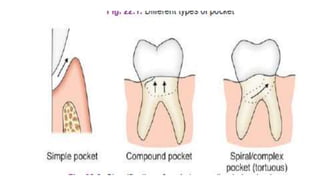
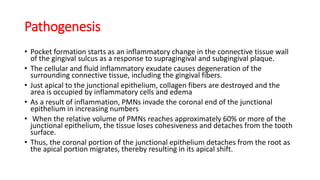
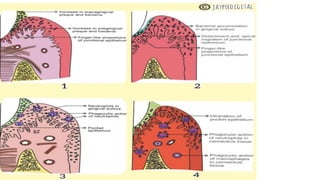
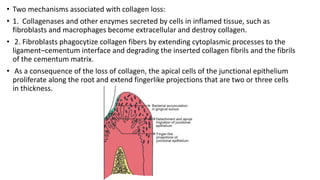
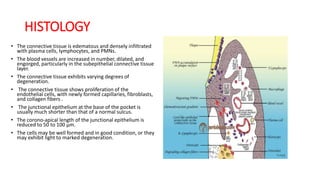
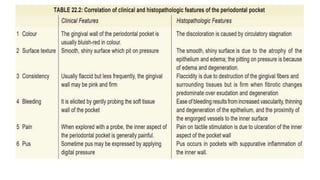
This document discusses periodontal pockets, including their definition, anatomy, classification, clinical features, pathogenesis, histology, clinical assessment, and management. A periodontal pocket refers to a pathologically deepened gingival sulcus, usually due to inflammation leading to the extension of gingivitis into periodontitis. Pockets are classified based on their morphology, number of tooth surfaces involved, disease activity, soft tissue wall characteristics, and lateral wall composition. Clinically, pockets present with symptoms like pain and signs like bleeding gums. Histologically, pockets show inflammation and connective tissue degeneration. Pockets are assessed clinically using probes and radiographically using markers. Management involves surgical procedures like raising periodontal flaps





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


