
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Periodontal Pocket.pptx
Similar to Periodontal Pocket.pptx (20)
More from DentalYoutube
More from DentalYoutube (20)
Recently uploaded
Recently uploaded (20)
Periodontal Pocket.pptx
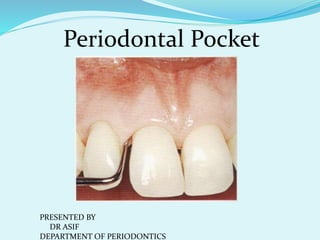
- 1. Periodontal Pocket PRESENTED BY DR ASIF DEPARTMENT OF PERIODONTICS
- 2. Def : Pathological deepening of gingival sulcus. Classification : •Gingival : Relative or false •Periodontal: True
- 3. Classification of periodontal pockets i. Depending on base of the pocket: A. Suprabony : Supra crestal, Supra alveolar B. Infrabony : Intrabony, Intra alveolar
- 5. ii. Based on involved tooth surfaces : A. Simple B. Compound C. Complex
- 6. 6 Depending upon nature of soft tissue wall of pocket : Pockets Edematous Fibrotic
- 7. 7
- 8. 8 Depending upon the disease activity : Pockets Active Inactive
- 10. CLINICAL FEATURES : Bluish red thickened marginal gingiva. Bluish red vertical zone from gingival margin to alveolar mucosa. Suppuration with gingival bleeding. Tooth mobility with diastema formation. Generally asymptomatic, but less frequently associated with localized deep dull pain sensitivity Urge to bite on the affected area Urge to use toothpick or needles relief after bleeding is induced
- 13. POCKET CONTENTS : Micro organisms and their byproducts Dental plaque GCF, Salivary mucin Food remnants Desquamated epithelial cells Leukocytes DIAGNOSIS : Williams graduated periodontal probe.
- 14. Difference between Suprabony and Infrabony pockets : •Base of the pocket •Type of bone loss •Transeptal fibers arrangement •Remaining PDL fibers
- 15. Pathogenesis of pocket formation: Pockets are caused by bacteria and their toxic byproducts. Toxic byproducts cross the epithelial barrier and produce pathological changes in the connective tissue, ultimately leading to deepening of gingival sulcus Sequence of events in progression of periodontal pockets: •Bacterial byproducts induce inflammatory changes in connective tissue of gingival sulcus. •The cellular and fluid inflammatory exudate causes degeneration of connective tissue. •Just apical to JE an area of destroyed collagen fiber develops and gets occupied by inflammatory cells and exudates.
- 17. •Destruction of collagen fibers take place by two mechanisms : An enzyme collagenase is released by PMN’s and Macrophages Bacterial enzymes induce cytotoxic changes in fibroblasts These altered fibroblasts phagocytose collagen and resorb gingival fibers •Due to continuous loss of collagen the apical JE proliferates along the root. •Hence the coronal JE detaches from the root. •More no of PMN’s from connective tissue invade the coronal end of JE. •Once the relative volume o PMN’s exceed by 60%, the tissue looses cohesiveness and detaches from tooth surface. •Thus the sulcus shifts apically. Plaque Gingival inflammation Pocket formation More plaque formation
- 18. 18 Due to inflammation PMNs invade coronal end of the junctional epithelium Relative volume of PMNs reaches approximately 60% or more of the junctional epithelium Tissue loses cohesiveness and detaches from the tooth surface. --- detaches from the root --- migrates, resulting in its apical shift --- gradually occupies an increasing portion of the sulcus lining Coronal portion Apical portion Oral sulcular epithelium
- 19. 19 Extension of junctional epithelium along root requires presence of healthy epithelial cells. Continued inflammation Gingiva increases in bulk Crest of gingival margin extends coronally Apical cells of junctional epithelium continue to migrate along root Coronal cells continue to separate from it Epithelium of lateral wall of the pocket proliferates to form bulbous, cordlike extensions into inflamed connective tissue Leukocytes and edema from inflamed connective tissue infiltrate the epithelium --- resulting in degeneration and necrosis.
- 20. HISTOPATHOLOGY 1. Soft tissue wall 2. Root surface wall
- 21. 1. Soft tissue wall (CT) : CT is edematous, densely infiltrated with plasma cells, lymphocytes, scattering of PMN’s. Blood vessels are increased, dilated and engorged. CT exhibits varying degrees of degeneration and proliferation of endothelial cells, newly formed capillaries and collagen fibers. JE is usually much shorter with coronoapical length of 50-100 micro meters. Cells of JE are in good condition or show slight vacuolar degeneration.
- 22. The lateral wall (sulcular epithelium) shows severe degenerative changes. Epithelial cells undergo vacuolar degeneration and necrosis of epithelium. This leads to ulceration of lateral wall, exposure of inflamed CT and suppuration. Bacterial invasion is seen in the apical and lateral wall of pocket. Bacterial invasion is active or by passive translocation. They invade Intercellular spaces Deeper epithelial cells Basement laminaSubepithelial CT. Prominent microorganisms are GM –ve like PG, PI, AA.
- 23. 3. Root surface changes: cause pain, perpetuate infection, complicate periodontal treatment. Structural changes: •Degeneration of collagen fibrils. •Penetration of bacteria. •Presence of pathologic granules(incomplete mineralization) •Necrotic cementum.
- 24. Chemical changes: •Areas of increased mineralization(ca,mg,po,fl.)increased hardness. •Areas of decreased mineralization Root caries. •Root caries appears as yellowish or light brown. •Progression is around root rather than into root. •Aa is dominant microorganism.
- 25. Cytotoxic changes: •Bacterial endotoxins are present on root surfaces. •Prevents attachment of normal fibroblasts. •Induce inflammatory reaction, when re implanted in mucosa even when autoclaved.
- 26. Periodontal disease activity: Related to specificity of plaque. Periods of exacerbation: Increased inflammatory response. Increased bleeding and exudate. Increased bone,CT, PDL loss. Periods of quiescence: Decreased above conditions. Site specificity: Affected and non affected sites coexist. Periodontal pockets and pulp changes: Produce significant pulp changes through lateral canals or periapically. Severe pain.
- 28. Periodontal pockets as healing lesions: •These are chronic lesions. •Constantly undergo repair •Presence of plaque does not allow complete healing. •Clinical presentations of gingival features are dependent on predominance of destructive or repair phase.
- 29. Relation of CAL and bone loss with pocket depth. CAL is distance between CEJ to base of pocket. Pocket depth is distance between gingival margin and base of pocket.
- 31. Periodontal Abscess : (Lateral or Parietal abscess) Localized purulent inflammation in periodontal tissues.
- 32. Periodontal abscess : An acute destructive process in the periodontium resulting in localized collection of pus and not arising from pulp Classification Location Onset & course of action Number of Abscess
- 34. Symptoms : Pain Gingival and mucosal pain Red to reddish blue gingiva Teeth are tender on chewing and sensitive to percussion Mobility May have sinus tract and already draining Lymphadenopathy and slight elevation of body temperature Purulent exudate
- 35. Microscopic features : •Presence of viable and non viable PMN’s. •PMN’s liberates enzymes that digest cells and other tissue structures. •Liquid pus is formed. •Acute inflammation surrounds this purulent area. •Epithelium exhibits intra and extra cellular edema and invasion of leucocytes.
- 37. ETIOLOGY : Periodontitis related cases Pockets with tortuous course. Incomplete removal of calculus during periodontal treatment. Partial treatment resulting in coronal occlusion and purulent bacteria remain deep inside the pocket particularly deep narrow and tortuous pocket Use of oral irrigation devices that may push bacteria deep into tissues Antibiotics without debridement in advanced periodontitis
- 38. Etiology : Non periodontitis related Perforation during endodontic therapy Cracked tooth, vertical tooth fracture, external root resorption Impaction of tooth brush bristle, ortho elastics, dental floss, fish or chicken bone Microbial picture Anaerobic microorganisms, gm –ve like bacteroides melaninogenicus, capnocytophaga, PG, PI fungi spirochetes, AA Microbial picture is similar to chronic periodontitis
- 39. Differential diagnosis: Periapical abscess: Deep caries, restorations, crowns, nonvital pulp Radiolucency at apex Pain in the apex of root Absence of periodontal pocket Severe pain on percussion Pain is sharp, intermittent ,severe and diffuse, not able to recognize affected teeth
- 40. Acute pulpitis: Most of the symptoms of periodontal abscess are absent except pain No soft tissue swelling are or purulent drainage Pain in opp arch affected by thermal changes Incomplete tooth fracture Pain or sensitivity on biting and sensitivity to cold
- 41. Treatment : Drainage through incision or through gingival sulcus Use of antimicrobial agents Open approach with flap surgery and osseous correction Irrigation with sterile saline, 0.1 % povidone iodine or 3 % hydrogen peroxide For systemic symptoms antibiotics and analgesics
- 42. Use of antibiotics: Culture and sensitivity 250 mg of tetracycline every six hours for 10 days 100 mg doxy once for 10days 500mg azithromycin single dose on first day followed by 250 mg once for 3 days 500/ 125 amox + clavulinic acid every 8 hour for 8 days 500mg metronidazole every 8 hour for 10 days 150 to 300 mg clindamycin 3 times for 7 days