5. Introduction
• DG is a clinically relevant entity…..
• DG can be associated with a wide range…..
• Because the majority of disorders causing DG…..
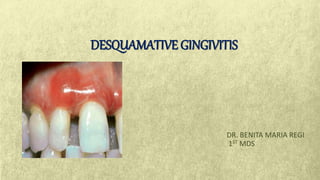
6. • Chronic desquamative gingivitis is characterized by intense redness and
desquamation of the surface epithelium of the attached gingiva.
Chronic desquamative gingivitis
7.
8. Etiology
• Dermatological diseases
• Endocrine disturbances
• Abnormal responses to
bacterial plaque
• Chronic infections
• Idiopathic
• Aging
(“desquamtive gingivitis- a clinical sign in mucous membrane pemphigoid: report of case and review of literature:
shamimul hassan”)
10. Epidemiological features
Pemphigus
vulgaris – 3%
to 15%
Oral lichen
planus – 24%
to 45%
Mucous
membrane
pemphigoid –
35% to 48%
“(Diagnostic Pathways and Clinical Significance of Desquamative Gingivitis
Lucio Lo Russo et al”)
11. Diagnosis of desquamative gingivitis:
Clinical
history
Clinical
examination
Biopsy
Microscopic
Examination
Immunofluore-
scence
13. Treatment
∆ Local treatment
Plaque control
Use of corticosteroid ointments and creams
∆ Systemic treatment
High dose therapy
Moderate dose
therapy
18. ORAL MANIFESTATIONS:
Radiating white or gray, velvety, thread-like papules in
a linear, annular or retiform arrangement forming
typical lacy, reticular patches, rings and streaks over
the buccal mucosa, lips, tongue and palate.
Vesicle and bulla formation.
21. DI- Linear-fibrillar deposits of fibrin in thebasement membrane zone.
Scattered immunoglobulin-staining cytoid bodies in the upper areas of the lamina
propria.
Serum tests using indirect immunofluorescenceare negative in lichenplanus.
22. TREATMENT:-
The keratotic lesions of oral lichen planus are asymptomatic and do not
require treatment.
The erosive, bullous, or ulcerative lesions of oral lichen planus are treated with high-
potency topical steroid such as 0.05% fluocinonide ointment (Lidex, three times daily).
It can also be mixed 1:1 with carboxymethyl cellulose (Orabase) paste or other adhesive
ointment.
23. • SEVERE CASES - Intralesional injections of triamcinolone acetonide (10 to 20 mg) or
short-term regimens of 40 mg prednisone daily for 5 days followed by 10 to 20 mg
daily for an additional 2 weeks.
• Topical tacrolimus
24. PEMPHIGOID
Cutaneous, immune-mediated, subepithelial bullous diseases that are
characterized by a separation of the basement membrane zone, including
bullous pemphigoid pemphigoid
gestationis
mucous membrane
pemphigoid
25. Cicatricial pemphigoid.
Chronic, vesiculobullous autoimmune disorder
It predominantly affects women in fifth decade of life.
Five subtypes:-
28. ORAL MANIFESTATIONS
• Desquamative gingivitis with areas of
erythema, desquamation, ulceration, and
vesiculation of the attached gingiva.
• Bullae- thick roof- rupture in 2-3 days
leaving irregular shaped areas of ulceration;
healing- 3 weeks or longer.
29. • Separation of epithelium and C.T.occursatthebasementmembranezone.
• EM- shows spilt in basal lamina
31. • Topical steroids – main Rx for mucous memb. Pemphi.
• Fluocinonide(0.05%) and Clobetasol propionate (0.05%) in an adhesive
vehicle can be used 3 times a day for 6 mnths.
33. Oral Manifestations
• Oral lesions – less frequently in BP than in CP
• Presence of vesicles and areas of erosion and ulceration
• Lesion- painful
• Gingival tissues appear extremely erythematous….
Bullae on gingiva
35. IgG&C3 immune deposits along epithelial basement membrane and circulating IgG
antibodies to the epithelial basement membrane.
Direct immunofluorescence is positive in 90% to 100% of these patients, whereas
indirect immunofluorescence is positive in 40% to 70% of affected patients
36. • control signs and symptoms
• Primary Rx –moderate dose of systemic prednisone
• Steroid sparing strategies (Prednisone + immunomodulatory drugs)…
• For localized lesions of bullous pemphigoid,….
37. • PEMPHIGUS - Group of autoimmune bullous disorders - cutaneous and/or mucous
membrane blisters
Types
P. vulgaris P. foliaceous
P. vegetans
P. erythematosus
38. • Lethal chronic condition
• Predilection in women(after 4th decade of life)
39.
40. • Range from small vesicles to large bullae
• Rupture of bullae leads to extensive areas of
ulceration
• Any area of oral cavity involved- Oral
lesions confine less often to gingival
tissues
• Nikolsky’s sign….
ORAL LESIONS:-
Soft palate > buccal mucosa > tongue > lower labial mucosa > gingiva
43. TREATMENT
• Systemic corticosteroids with or without other immunosuppressive agents
• Steroid sparing therapies- pt not responsive to corticosteroid.
• Optimal oral hygiene
• Pts in maintenance phase- prednisone before oral prophylaxis and periodontal surgery
to prevent flare ups.
44. CHRONIC ULCERATIVE STOMATITIS
• 1990
• Condition presents with chronic oral ulcerations
• Predilection for women(4th decade)
• Erosions and ulcerations in oral cavity- few cases
with cutaneous lesions
ORAL LESIONS
•Painful, solitary small blisters and erosions with surrounding erythema – mainly
on gingiva and lateral border of the tongue ; hard palate may also present similar
lesions.
45. TREATMENT
• Mild cases- topical steroids (fluocinonide, clobetasol propionate) and topical
tetracycline
• Severe cases- systemic steroids
• Hydroxychloroquine sulfate 200-400 mg/ day – Rx of choice for complete,
long lasting remission
46. LINEAR IgA DISEASE (LINEAR IgA DERMATOSIS)
• Uncommon mucocutaneous disorder with
predilection in women
C/F
• Pruritic Vesiculo bullous rash, during middle to
late age..
47. ORAL LESIONS
• Vesicles, Painful ulcerations or erosions and erosive gingivitis/chelitis
• Hard and soft palate commonly affected →
tonsillar pillars, buccal mucosa, tongue and gingiva
• Rarely, oral lesion may be the only manifestation for several years; before
cutaneous lesions
48. Combination of
Sulfones and
Dapsone
Small amounts of
Prednisone (10-
30mg/day) canbe
added
tetracycline
(2g/day)
combined with
nicotinamide (1-
5g/day)
Mycophenolate(1g
twice daily) +
prednisolone
(30mg daily)
49. Chronic condition
Young adults (20-30years)
Slight predilection formales.
Bilateral and symmetric pruriticpapules/vesicles…
Oral lesions - Painful ulcerations preceded by collapse of ephemeral
vesicles/bullae to erythematous lesions.
50. HISTOPATHOLOGY
Focal aggregates of neutrophils and eosinophils amidst deposits of fibrin at the apices
of the dermal pegs.
IMMUNOFLUORESENCE
Direct immunofluoresence show that IgA &C3 are present at the dermal papillary apices.
There is clear association with celiac disease & circulatory anti endomysial and anti
gliaden antibodies may be of diagnostic value.
59. • Target or iris lesions with central clearing
Oral lesions
• 70% of patients with skin involvement (McCarthy 1980)
• Multiple, large, painful ulcers with an erythematous border
• Hemorrhagic crusting of vermilion border of lips
60. Buccal mucosa > tongue >lower labial mucosa > floor of the mouth > palate > gingiva.
61. Steven Johnsons Syndrome
• Severe bullous form
• Abrupt occurrence of fever, malaise, photophobia and
eruptions of oral mucosa, genitilia and skin
• Oral lesions → rupture → surfaces covered with thick white
or yellow exudate
• Lips - ulceration with bloody crusting
• ANUG
63. DRUG ERUPTIONS
• Drug acts as an allergen either alone or in combination, sensitizes the tissues and
then causing the allergic reaction.
• TYPES
- Stomatitis medicamentosa - mouth or parenterally
- Stomatitis venenata(contact dermatitis) – local use.
70. Clinical significance
• Painful gingival and oral lesions…..
• This can increase the inflammation associated with DG lesions,….
• The potential direct effects of DG-associated disorders on periodontal status have been investigated
rarely.
71. • It seems that the presence of DG lesions….
• In addition, systemic/topical…..
• Oral hygiene procedures should be performed avoiding trauma because many immune-mediated
disorders associated with DG are characterized by the Koebner phenomenon,
72. • Systemic complications also are important…..
• Systemic corticosteroids and/ or other immune suppressive drugs….
• A small but increased risk for malignant transformation of the oral mucosa….
“(Diagnostic Pathways and Clinical Significance of Desquamative Gingivitis
Lucio Lo Russo et al”)
73. • From a theoretic point of view, disorders causing DG may have potential harmful
• In fact, DG lesions are typically chronic and often associated to a wide range of oral
symptoms….
• In the instance of such an indirect effect…..
74. • On the other hand, a direct effect of DG lesions on periodontitis …..(Kornman, 2008).
• Immune-inflammatory mechanisms are also critical for the pathogenesis of most of DG-associated
disorders (Lo Russo et al, 2008), which often involves common molecules⁄cytokine networks [e.g. TNF-
a for OLP (Sugerman et al, 2002; Sugermann et al, 1996; Khan et al, 2003)].
75. • (Tricamo et al, 2006) showed that…...
• (Akman et al, 2008)…..
78. references
•Carranza clinical periodontology 12th edition
•Shafer's oral pathology 5th edition
•Diagnostic Pathways and Clinical Significance of Desquamative Gingivitis
J Periodontol 2008;79:4-24.
•Position Paper Oral Features of Mucocutaneous Disorders
J Periodontol 2003;74:1545-1556.
•Desquamative Gingivitis: Investigation, Diagnosis and Therapeutic Management in Practice
Perio 2005; Vol 2, Issue 3: 183–190
•Periodontal Implications: Mucocutaneous Disorders
Ann Periodontol 1996;1:401-438
• Desquamative Gingivitis − Aetiology, Diagnosis and Management;
Lewis Winning, Amanda Willis, Brian Mullally and Christopher Irwin
• Desquamtive gingivitis- a clinical sign in mucous membrane pemphigoid: report of case and review of
literature: Shamimul Hassan