Downloaded 54 times

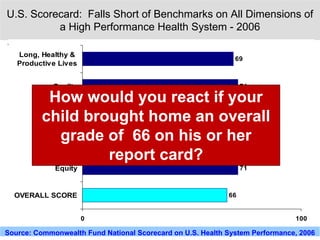
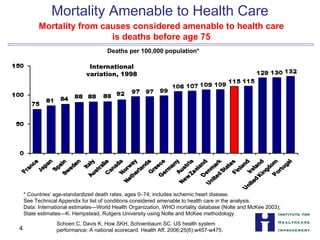




The document outlines significant deficiencies in the U.S. healthcare system, highlighting high rates of unreceived care, patient errors, and variations in mortality and costs compared to other countries. It introduces the 5 Million Lives Campaign, aiming to reduce incidents of harm in healthcare by engaging thousands of hospitals and applying evidence-based interventions to improve patient safety. Success is deemed achievable with leadership commitment, clear goals, data transparency, and a culture of ownership among healthcare providers.