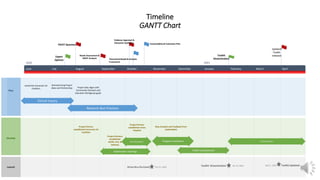
The DNP project presentation discusses barriers to influenza vaccination and proposes decreasing out-of-pocket costs to increase rates. It analyzes the vaccination system at ACHN, finding gaps in access due to limited free vaccines. A drive-thru flu clinic is proposed where uninsured individuals get free vaccines and insured pay nothing. The goals are to increase adult vaccination rates at ACHN by 50% by February 2021 and create a toolkit by April 2021 to enable replication and progress toward the Healthy People 2030 goal.







![Literature review
Levels of Evidence Synthesis Table
Level
1 2 3 4 5 6 7 8 9 10 11 12 13
Level I: Randomized controlled trial (RCT) or Systematic review of
RCTs
Level II: Systematic review of a combination of RCTs and quasi
experimental studies
Level III: Non-experimental study or Systematic review of a
combination of RCTs and non-experimental studies/non-
experimental studies only with or without meta -analysis
X X X X X X X X X
Level IV: Opinion of respected authorities and/or nationally
recognized expert committees or consensus panels based on
scientific evidence.
X
Level V: Based on experiential and non-research evidence
including quality improvement programs.
X X X
1 = Abbas et al., (2018); 2 = Akpalu et al., (2020); 3 = Bach et al., (2019); 4 =Falcone, (2019); 5 =Falcone et al., (2019); 6 =Husain et al., (2016); 7 =National Vaccine Advisory
Committee [NVAC], (2012); 8 =Okoro et al., (2017); 9 =Singh et al., (2020); 10 = Williams et al., (2017); 11 =Yeung et al., (2016); 12 =Community Preventative Services Taskforce
[CPSTF], (2015); 13 =CPSTF, (2014](https://image.slidesharecdn.com/dnpprojectpresentationnurs883-210124131310/85/Dnp-project-presentation-nurs-883-10-320.jpg)
![Outcomes Synthesis
, , —, NE, NR, 1 2 3 4 5 6 7 8 9 10 11 12 13
Outcome #1 – Influenza vaccine uptake in uninsured
adults
— NE NE NR NE NE NE NE
Outcome #2 – Influenza vaccine uptake in adults
(generalized)
NE NE
(insured)
NE
Outcome #3 – Healthcare cost savings/Benefit NE NE NE NE NE NE
Outcome #4 – Cost of Intervention/Expenditure NR NR NR NR NR NR NE NR NE NE
Outcome #5 – Morbidity NE NE NE
Outcome #6 - Mortality NE NE NE NE
SYMBOL KEY
↑ = Increased, ↓ = Decreased, — = No Change, NE = Not Examined, NR = Not Reported
1 = Abbas et al., (2018); 2 = Akpalu et al., (2020); 3 = Bach et al., (2019); 4 = Falcone, (2019); 5 =Falcone et al., (2019); 6 = Husain et al., (2016); 7 = National Vaccine Advisory Committee
[NVAC], (2012); 8 = Okoro et al., (2017); 9 = Singh et al., (2020); 10 = Williams et al., (2017); 11 = Yeung et al., (2016); 12 = Community Preventative Services Taskforce [CPSTF], (2015);
13 = CPSTF, (2014)](https://image.slidesharecdn.com/dnpprojectpresentationnurs883-210124131310/85/Dnp-project-presentation-nurs-883-11-320.jpg)