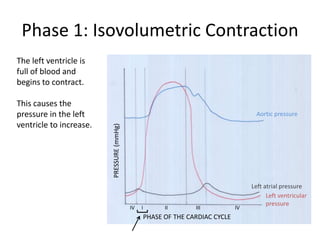
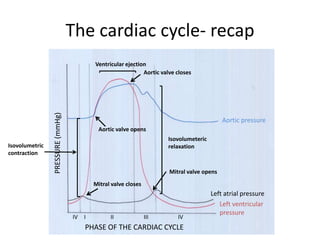
The cardiac cycle consists of 4 phases:
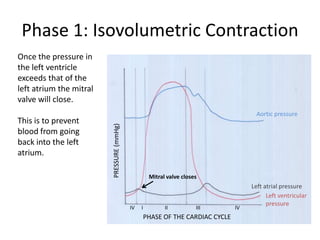
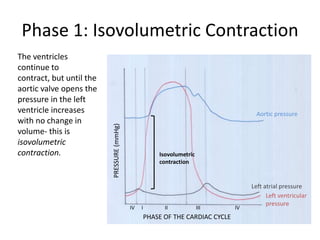
1) Isovolumetric contraction - the ventricles contract but volume remains constant until the aortic valve opens
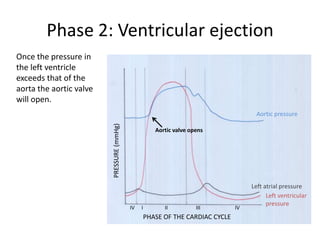
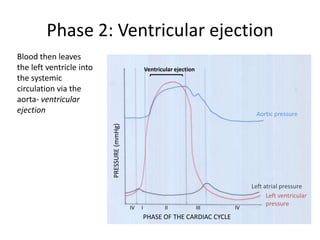
2) Ventricular ejection - the aortic valve opens and blood is ejected from the ventricles into the aorta
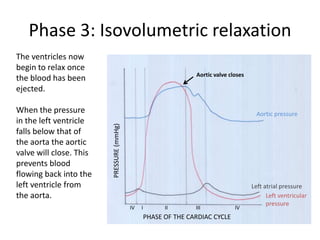
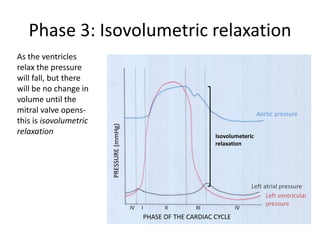
3) Isovolumetric relaxation - the ventricles relax but volume is constant until the mitral valve opens
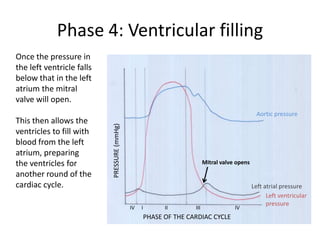
4) Ventricular filling - the mitral valve opens and the ventricles fill with blood from the atria in preparation for the next cycle.