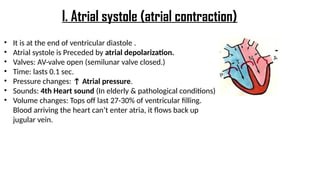
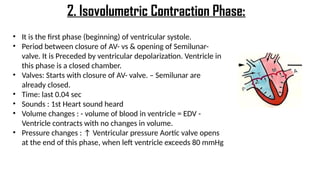
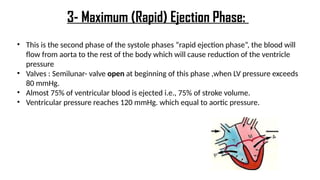
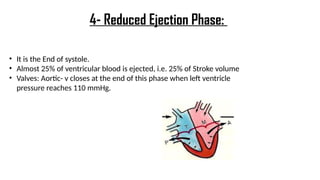
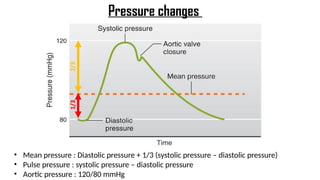
The document presents a detailed overview of the cardiac cycle, describing the heart's main functions, the sequence of mechanical and electrical events during each heartbeat, and the roles of valves and pressures. It outlines the phases of systole and diastole, providing insights into the timing and significance of each phase for blood flow and heart function. Additionally, it explains heart sounds and their relation to valve closures and atrial pressure changes during the cycle.