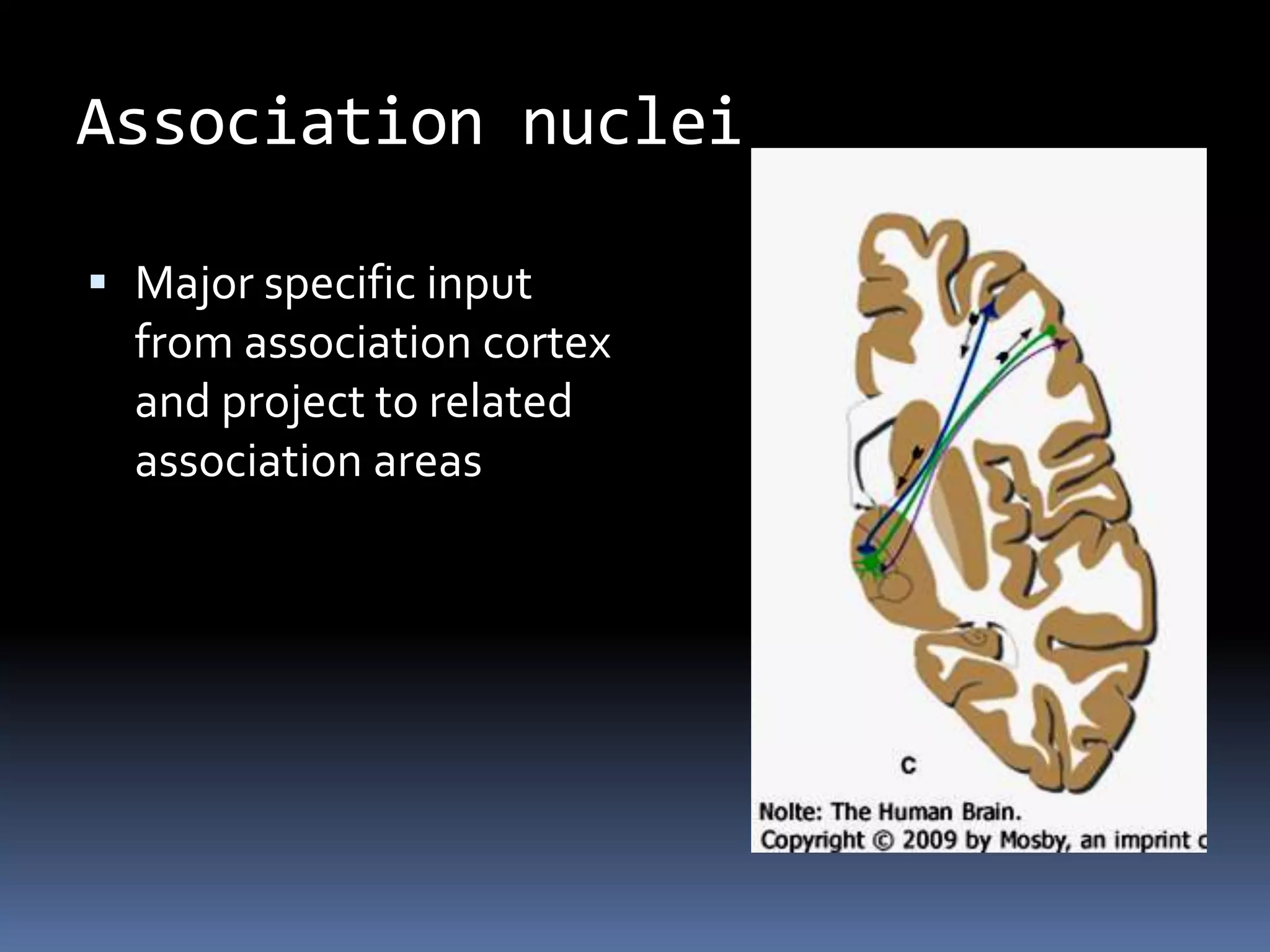
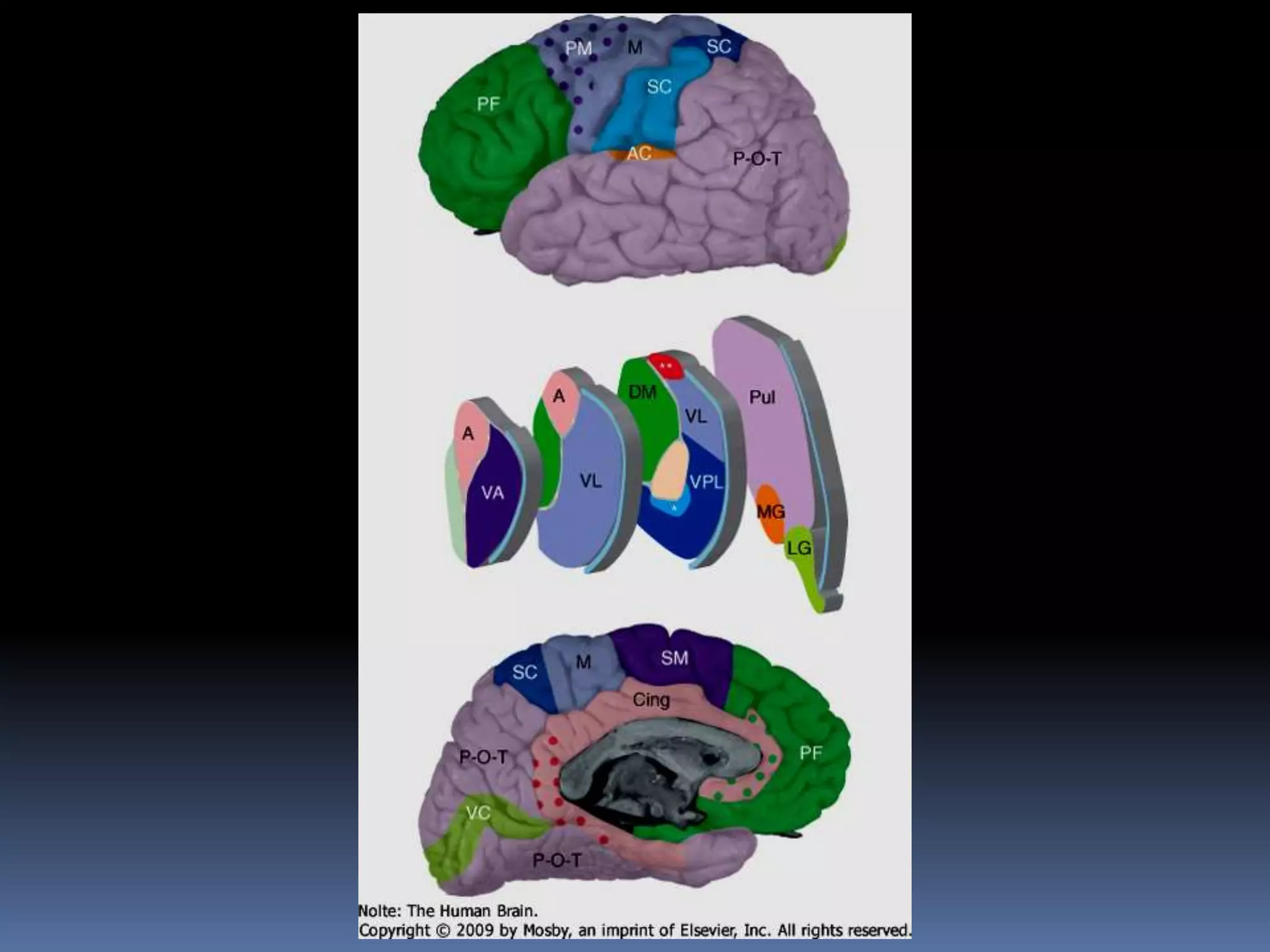
The thalamus acts as a relay center and gatekeeper for sensory and motor information between subcortical structures and the cerebral cortex. It is divided into nuclear groups based on inputs and outputs. Relay/specific nuclei receive defined inputs and project to specific cortical areas, transmitting information like touch, sound and vision. Association nuclei connect association areas and are involved in higher-level processing. Nonspecific nuclei like the intralaminar and reticular nuclei project widely and regulate arousal and cortical activity. Damage to posterior thalamic areas can cause thalamic syndrome with abnormal sensory experiences and central pain.




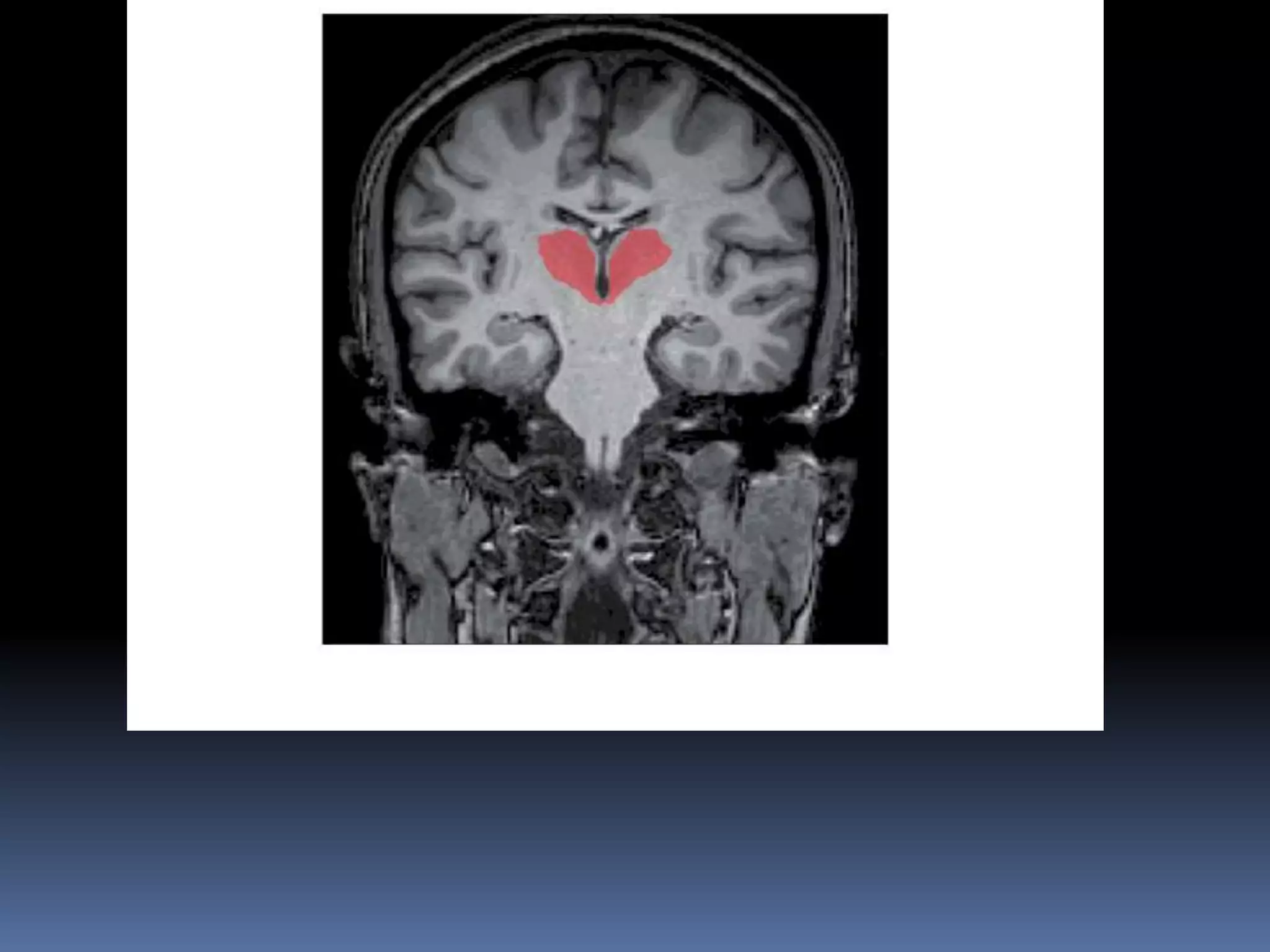







![Nuclei of ventral tier
Ventral anterior, ventral lateral- concerned
with motor control; are connected to basal
nuclei and cerebellum
Ventral posterior is subdivided into ventral
posterolateral[ smatosensory input from
body] and ventral posteromedial
[somatosensory input from head]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-22-2048.jpg)



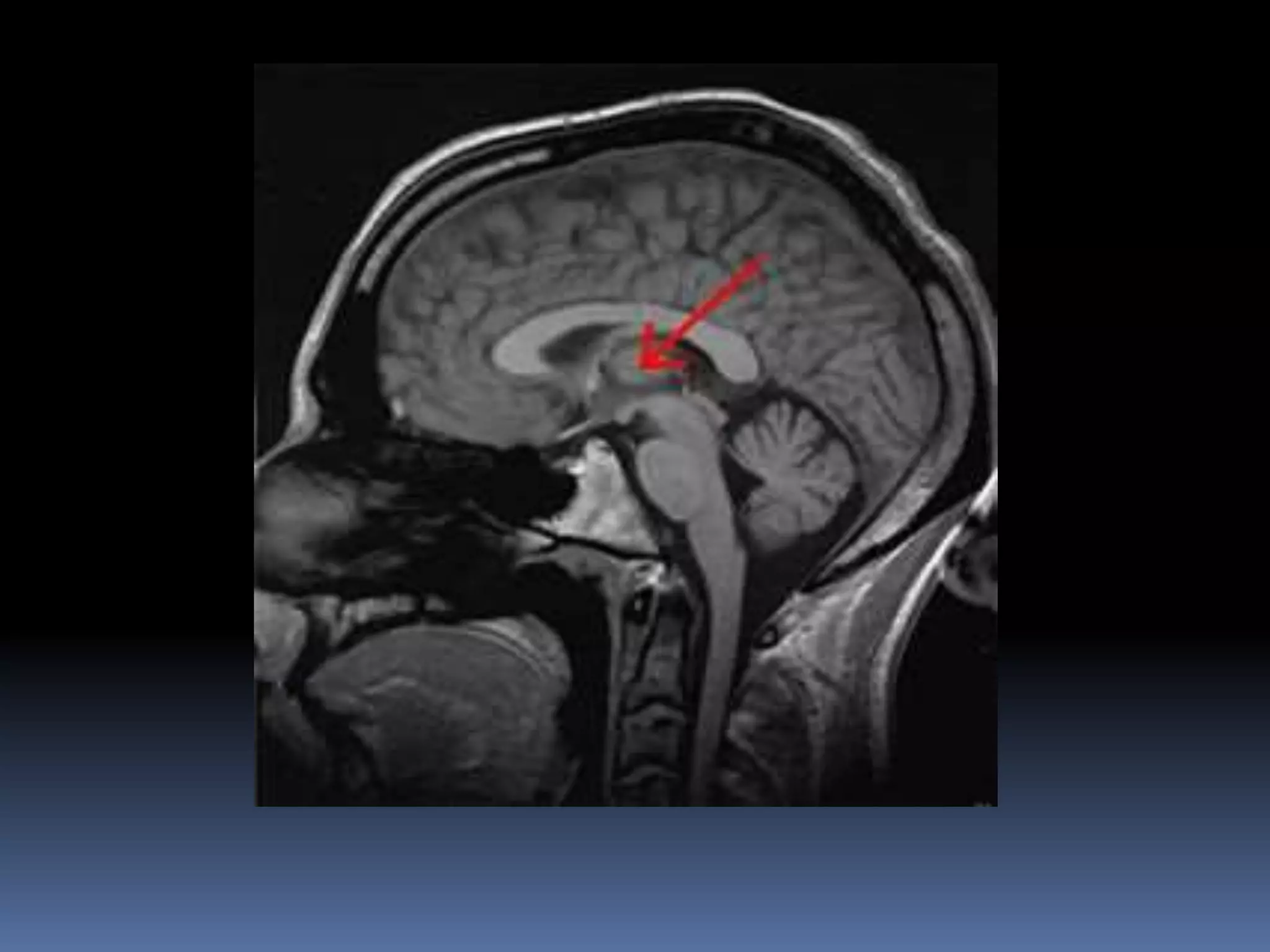
![Midline nuclei
Rostral continuation of periaqueductal gray
matter
Form interthalamic adhesion [when present]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-26-2048.jpg)
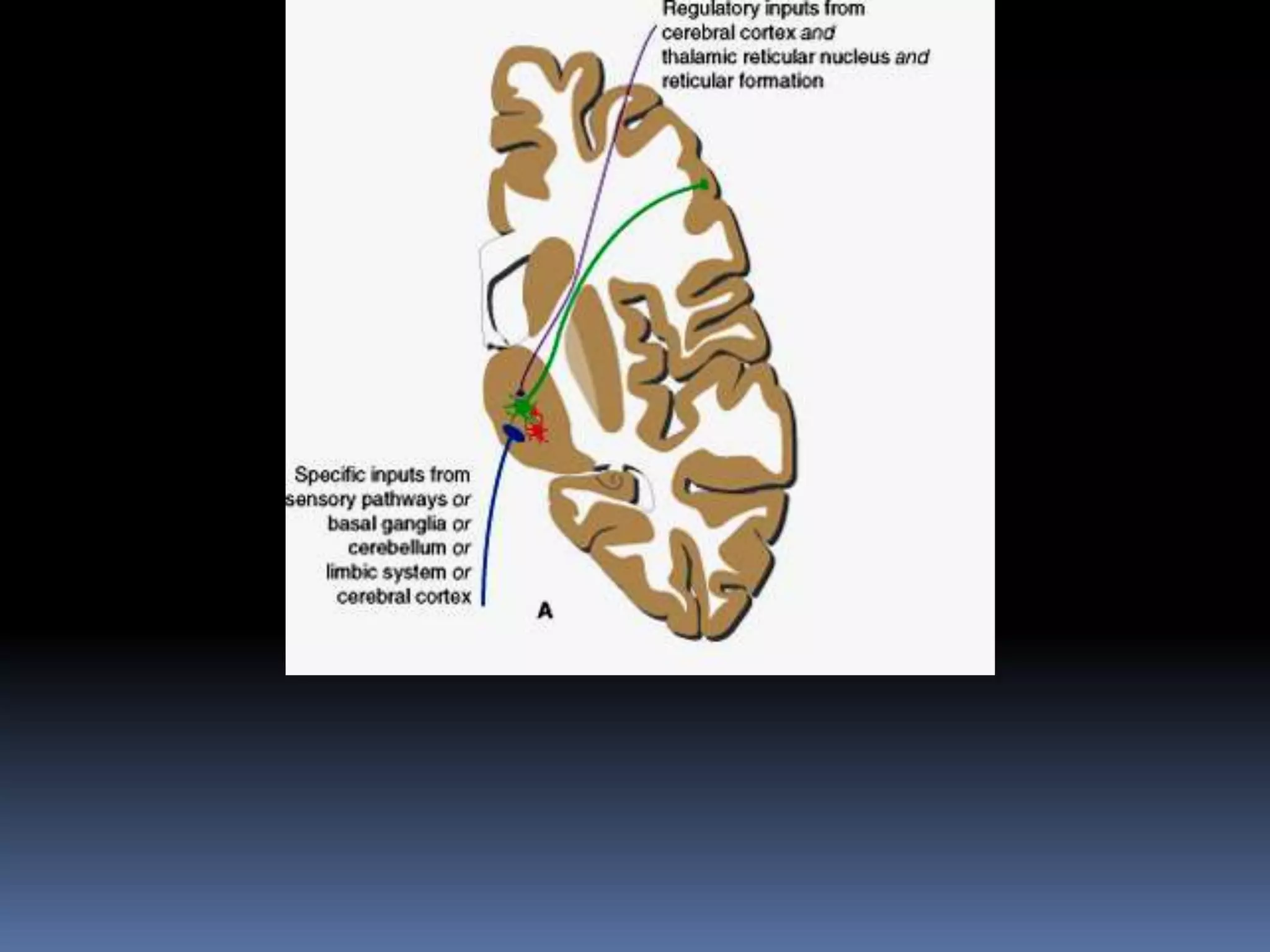
![Inputs
Specific - Regulatory
Specific inputs convey information that a
given nucleus may pass to cerebral cortex
[and for some nuclei to additional sites].
Examples; Medial lemniscus specifically to
VPL. Optic tract to LGB](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-28-2048.jpg)









![Relay/specific nuclei
Specific inputs from
subcortical areas[e.g.
medial lemniscus]-
project to a well
defined area of
cerebral cortex](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-49-2048.jpg)

![Ventral anterior
Input Output Functions
Pallidum [globus
pallidus]
Frontal lobe,
including premotor
and supplementary
motor areas
Motor planning and
more complex
behavior](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-51-2048.jpg)
![Ventral lateral [anterior
division]
Input Output Functions
Pallidum [globus
pallidus]
Premotor and
supplementary
motor areas
Planning
commands to be
sent to motor
neurons](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-52-2048.jpg)
![Ventral lateral [posterior
division]
Input Output Functions
Contralateral
cerebellar nuclei
Primary motor area Cerebellar
modulation of
commands sent to
motor neurons](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-53-2048.jpg)
![Ventral posterolateral
Input Output Functions
Medial lemniscus,
spinal lemniscus
Primary
somatosensory area
Somatic sensation
[principal pathway,
from contralateral
body below head]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-54-2048.jpg)
![Ventral posteromedial
Input Output Functions
Contralateral
trigeminal sensory
nuclei
Primary
somatosensory area
Somatic sensation
[principal pathway,
from contralateral
half of head: face,
mouth, larynx,
pharynx, dura
mater]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-55-2048.jpg)
![Medial geniculate body
Input Output Functions
Inferior colliculus Primary auditory
cortex
Auditory pathway
[from both ears]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-56-2048.jpg)
![Lateral geniculate body
Input Output Functions
Ipsilateral halves of
both retinas
Primary visual
cortex
Visual pathway
[from contralateral
visual fields]](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-57-2048.jpg)

![Lateral dorsal
Input Output Functions
Hippocampal
formation,
pretectal
area,superior
colliculus
Cingulate
gyrus,Parietal,
temporal, and
association
cortex[visual
cortex]
Interpretation of
visual stimuli;
memory](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-60-2048.jpg)

![Intralaminar and midline
nuclei/nonspecific
Specific inputs[basal
nuclei or limbic
structures] and ptoject
to cerebral cortex,
basal nuclei, limbic
structures](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-63-2048.jpg)
![Intralaminar nuclei
Input Output Functions
Cholinergic and
central nuclei of
reticular
formation,locus
coeruleus, collateral
branches from
spinothalamic tracts,
cerebellar nuclei,
pallidum
Extensive cortical
projections, especially
to frontal and parietal
lobes; striatum
Stimulation of cerebral
cortex in waking state
and arousal from
sleep;somatic
sensation, especially
pain [from
contralateral head
and body]; control of
movement](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-64-2048.jpg)




![THALAMIC SYNDROME[DEJERINE-ROUSSY SYNDROME]
Damage more or less restricted to the
posterior thalamus can cause a characteristic
type of dysesthesia that is somewhat similar
to trigeminal neuralgia
paroxysms of intense pain may be triggered
by somatosensory stimuli.](https://image.slidesharecdn.com/bsgug6gltyiyjrbb0spt-thalamus-2-230505154223-2bed9a87/75/Thalamus_2-ppt-71-2048.jpg)



























![080 - Neurology Physiology] Thalamus Anatomy & Function.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/080-neurologyphysiologythalamusanatomyfunction-241127085853-17b20927-thumbnail.jpg?width=640&height=640&fit=bounds)






















