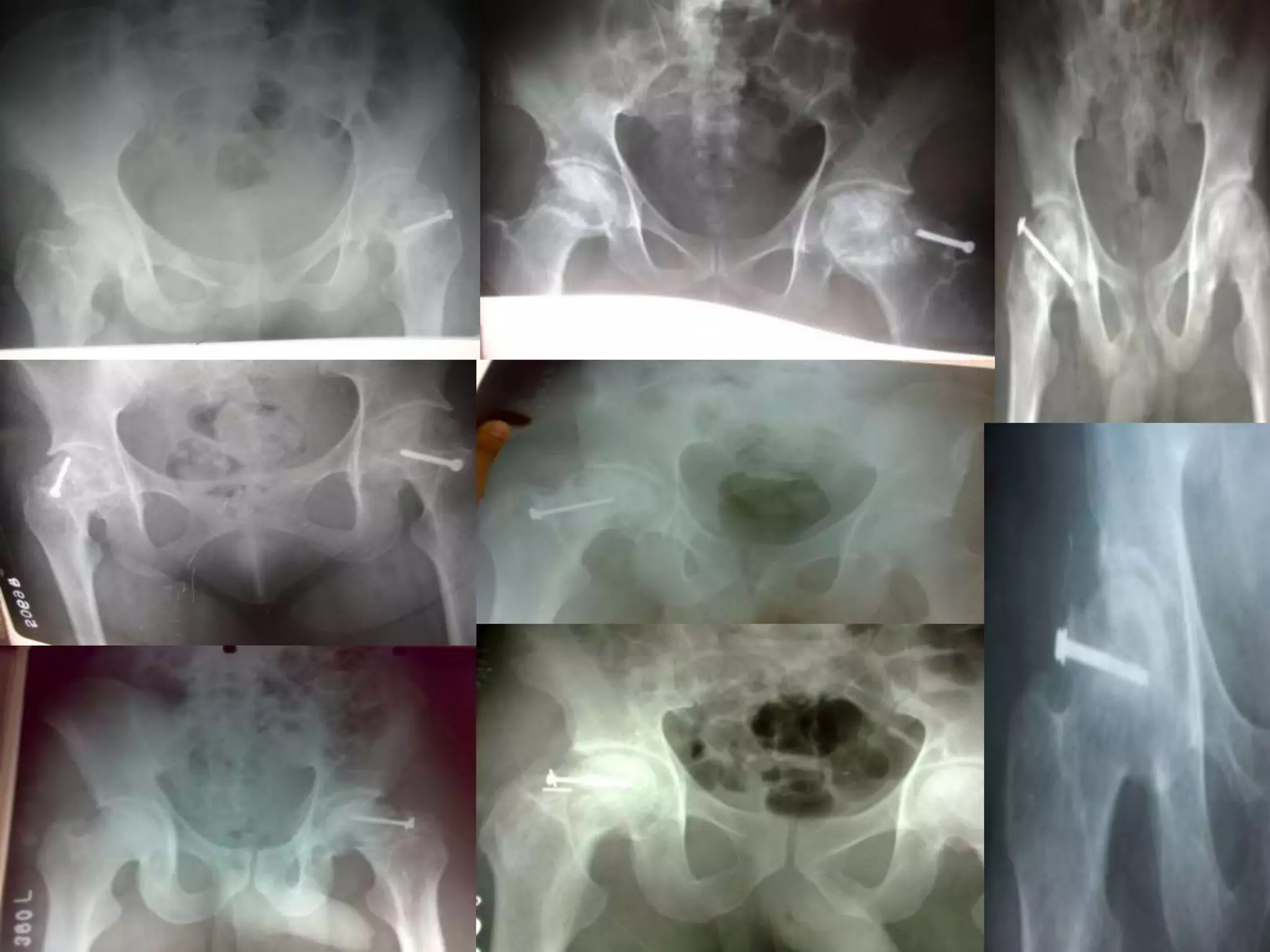
The document presents a study on the modified tensor fascia lata muscle pedicle graft (TFL MPG) for treating avascular necrosis (AVN) of the hip. It outlines the procedure's efficacy, revealing that all fifty patients experienced pain relief and improved mobility after treatment. The TFL MPG is highlighted as a viable biological option to reverse the pathology of AVN before significant joint collapse occurs.
![TENSOR FASCIA LATA
MUSCLE PEDICLE
GRAFT[TFL MPG] IN AVN hip
DR MOHAMED ASHRAF. Professor and head
drashraf369@gmail.com
DR Narayanan SK . Assistant professor
Govt TD medical college,alleppey,kerala,india](https://image.slidesharecdn.com/tensorfascialatatflmusclepediclegraftingforavnhip-drmohamedashraf-200909131544/75/Tensor-fascia-lata-tfl-muscle-pedicle-grafting-for-avn-hip-dr-mohamed-ashraf-hod-orthopaedics-govt-td-medical-college-hospital-alleppey-kerala-india-1-2048.jpg)


![• Presenting our long term
results of:
Modified TFL MPG
[tensor fascia lata
muscle pedicle graft]](https://image.slidesharecdn.com/tensorfascialatatflmusclepediclegraftingforavnhip-drmohamedashraf-200909131544/75/Tensor-fascia-lata-tfl-muscle-pedicle-grafting-for-avn-hip-dr-mohamed-ashraf-hod-orthopaedics-govt-td-medical-college-hospital-alleppey-kerala-india-4-2048.jpg)

























![MBBS [GMC CALICUT]
D ORTHO [GMCTRIVANDRUM]
MS ORTHO [MMC MADRAS]
DNB,MNAMS [NEW DELHI]
drashraf369@gmail.com](https://image.slidesharecdn.com/tensorfascialatatflmusclepediclegraftingforavnhip-drmohamedashraf-200909131544/75/Tensor-fascia-lata-tfl-muscle-pedicle-grafting-for-avn-hip-dr-mohamed-ashraf-hod-orthopaedics-govt-td-medical-college-hospital-alleppey-kerala-india-41-2048.jpg)




















































![Safe surgical dislocation[ssd] for avascular necrosis hip[ avn]](https://cdn.slidesharecdn.com/ss_thumbnails/safesurgicaldislocationssdforavascularnecrosishipavn-200914081007-thumbnail.jpg?width=640&height=640&fit=bounds)




![Osteoarticular tuberculosis [bone and joint tb] dr mohamed ashraf,hod orthopa...](https://cdn.slidesharecdn.com/ss_thumbnails/osteoarticulartuberculosisboneandjointtbdrmohamedashrafhodorthopaedicsgovttdmedicalcollegealleppeyke-200910130018-thumbnail.jpg?width=640&height=640&fit=bounds)





























