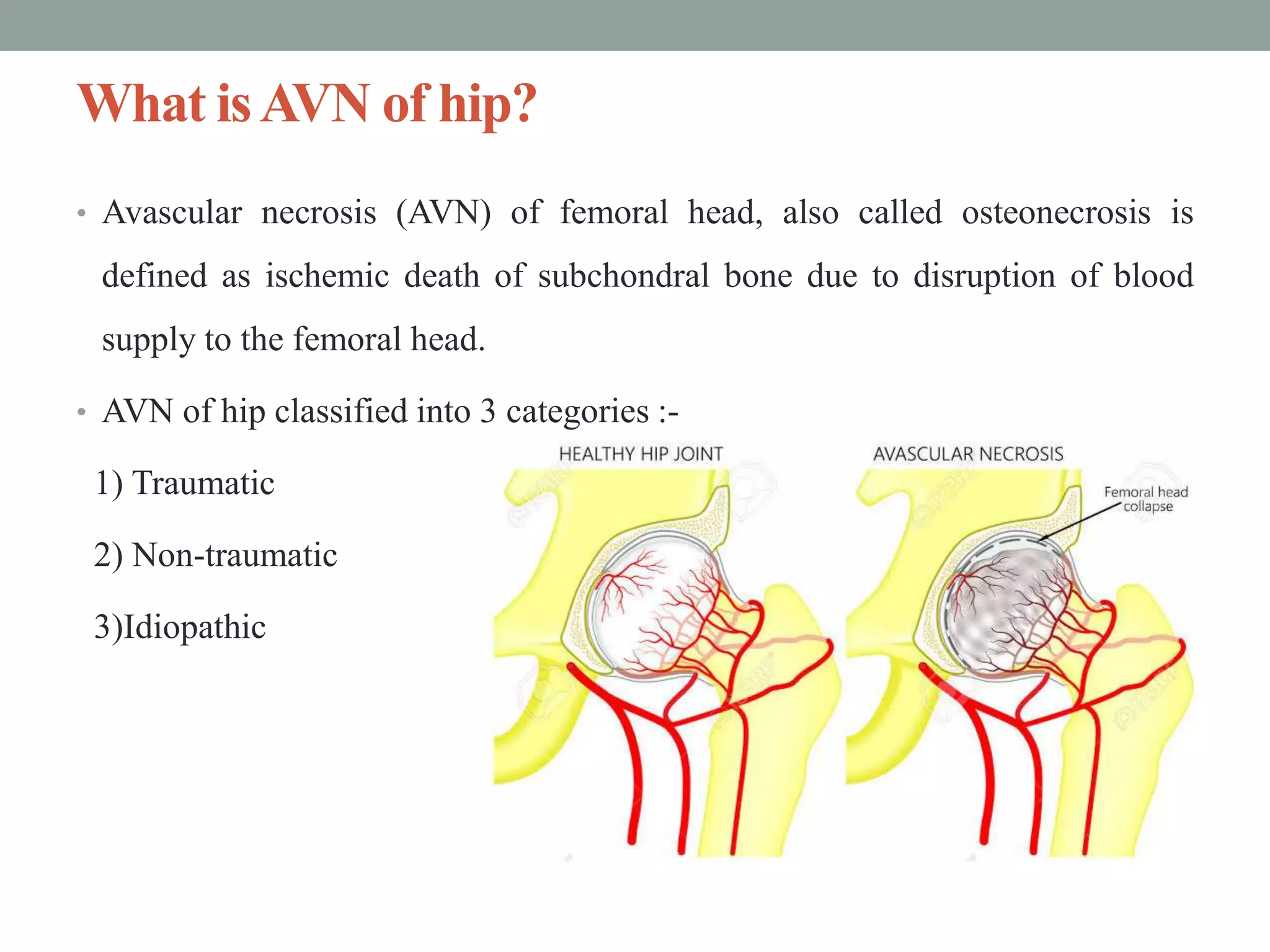
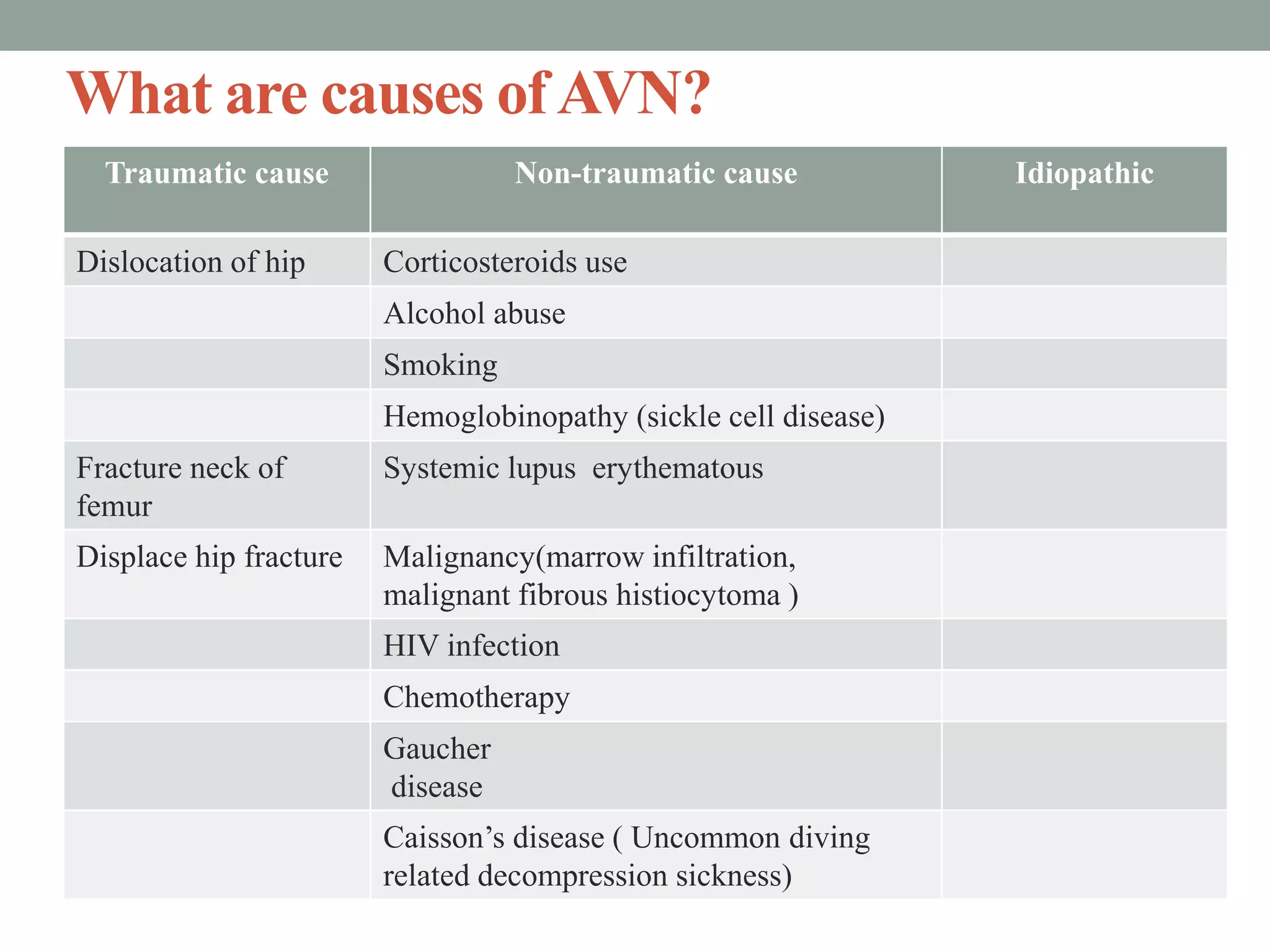
Avascular necrosis (AVN) of the hip, or osteonecrosis, is the ischemic death of the femoral head due to disrupted blood supply, categorized into traumatic, non-traumatic, and idiopathic causes. Diagnosis involves imaging techniques like MRI and X-rays, with a classification system that stages the disease based on symptoms and radiographic findings. Treatment varies based on the stage, ranging from conservative management and core decompression to surgical interventions such as osteotomy or total hip arthroplasty for advanced cases.

























![References
1. S. Brent Broadzman &Robert C. Manske, PT “Clinical Orthopaedic
Rehabilitation”- 3rd edition.
2. Jayant Joshi & Prakash Kotwal “ Orthopaedics and applied
Physiotherapy”- 3rd edition.
3. Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts
on osteonecrosis of the femoral head. World J Orthop 2015; 6(8): 590-601
[PMID: 26396935 DOI: 10.5312/wjo.v6.i8.590].
4. American Academy of Orthopedic Surgeons: http://orthoinfo.aaos.org](https://image.slidesharecdn.com/finalslidesharepppresentation-230824085630-0fdbe177/75/AVN-Of-Hip-pptx-28-2048.jpg)




































































