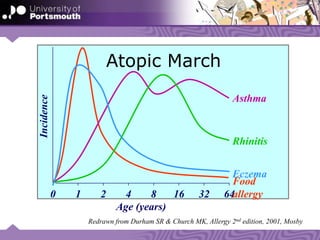
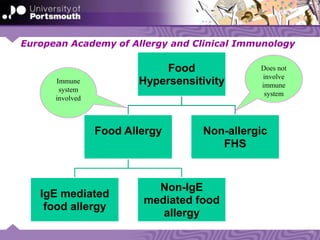
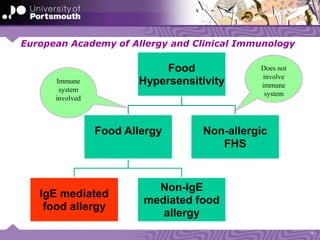






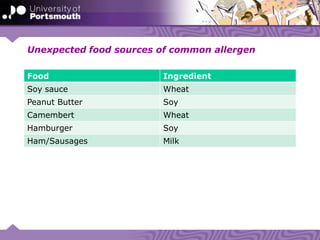



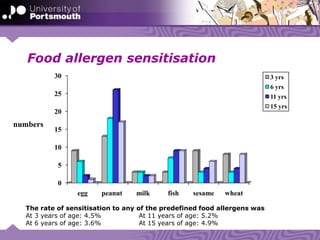


This document summarizes research on allergies conducted at the University of Portsmouth. It discusses various allergic diseases and their prevalence. Key points include: allergic diseases are becoming more common globally; atopy makes one more susceptible to allergies; the most common food allergies are to milk, eggs, peanuts, tree nuts, soy, wheat, fish and shellfish; and the FAIR study in the UK found self-reported food hypersensitivity in 10.9% of children, with confirmed food allergies between 1.4-2.9% depending on age based on food challenges.










































































































