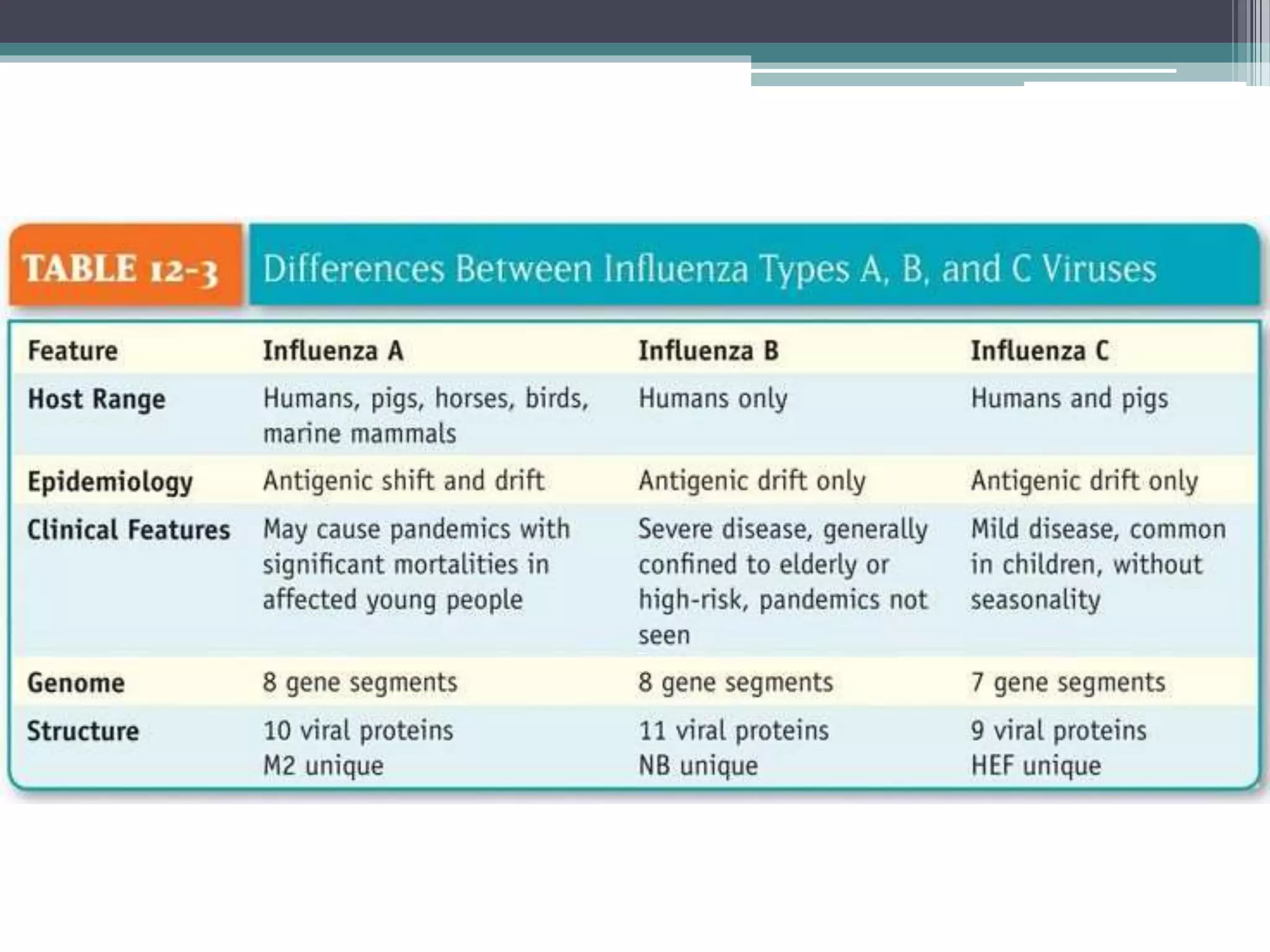
This document discusses swine flu, caused by the H1N1 influenza virus. It began as a pandemic in 2009 that spread to nearly every country and affected many people in India from 2009-2014. The virus is transmitted through respiratory droplets and can be shed for up to a week. Those at highest risk include young children, older adults, pregnant women, and those with chronic health conditions. The virus is an RNA virus from the Orthomyxoviridae family that undergoes genetic drift and shift. Clinical features include fever, sore throat, and myalgia. Complications can include pneumonia, encephalitis, and multi-organ failure.