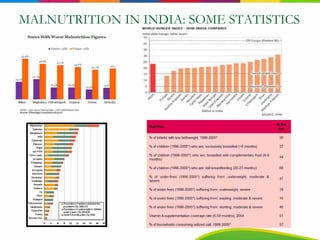
The document outlines India's serious problem with malnutrition, discussing statistics showing over 40% of underweight children globally are in India. It analyzes the current situation, noting India lacks a comprehensive national program and other nutrition programs do not fully address the problem. The document then proposes a national strategy and essential interventions to directly and indirectly combat malnutrition through improving nutrition, health services, sanitation, and more.




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















