Download as PDF, PPTX
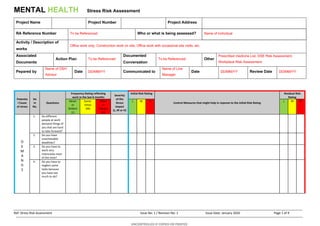

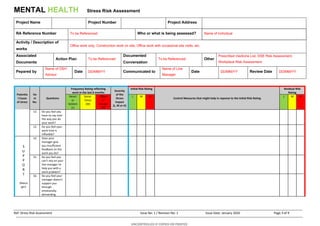
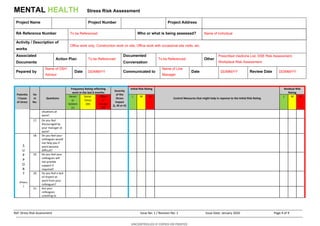
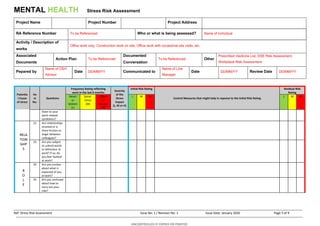
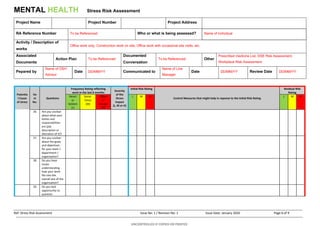
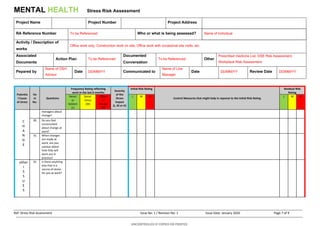
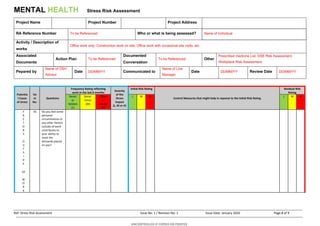
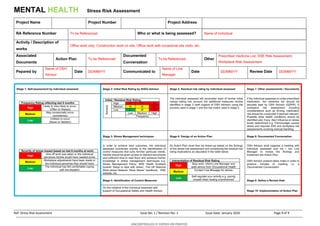

This document contains a mental health stress risk assessment form. It assesses potential causes of stress at work, including demands, control, support from managers and peers, relationships, role, and change. For each potential stressor, it evaluates the frequency and severity to determine an initial risk rating. It then considers control measures and residual risk ratings. The full process involves self-assessment, determining risk ratings, identifying stress management techniques, designing an action plan, documenting conversations, and setting a review date. The goal is to help manage work-related stress.



































































