Downloaded 197 times








![Crisis Cycle TCI TRAINING [30]](https://image.slidesharecdn.com/steve-vittos-assessing-and-treating-defiant-behavior-1209624284112203-8/85/Steve-Vittos-Assessing-And-Treating-Defiant-Behavior-75-320.jpg)
![Recovery Phase TCI TRAINING [6]](https://image.slidesharecdn.com/steve-vittos-assessing-and-treating-defiant-behavior-1209624284112203-8/85/Steve-Vittos-Assessing-And-Treating-Defiant-Behavior-76-320.jpg)
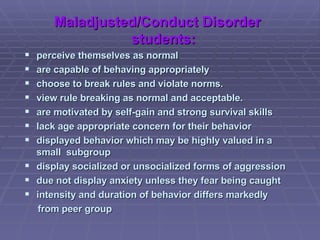
![When Young People Will Not Comply Actively listen and problem-solve Remove the others from the area Give choices and time to decide Let program consequences stand Redirect young person to a more attractive activity Appeal to the young person’s self-interest Use your relationship with the young person TCI TRAINING [33]](https://image.slidesharecdn.com/steve-vittos-assessing-and-treating-defiant-behavior-1209624284112203-8/85/Steve-Vittos-Assessing-And-Treating-Defiant-Behavior-77-320.jpg)
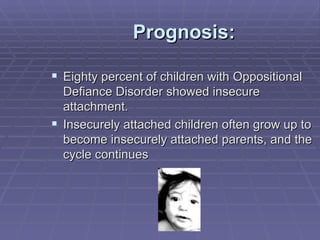
![I ASSIST I - Isolate the young person A - Actively listen S – Speak calmly, assertively, respectfully S – Statements of understanding precede requests I – Invite the young people to consider positive outcomes and behaviors S – Space reduces pressure T – Time helps young people respond to requests TCI TRAINING [43]](https://image.slidesharecdn.com/steve-vittos-assessing-and-treating-defiant-behavior-1209624284112203-8/85/Steve-Vittos-Assessing-And-Treating-Defiant-Behavior-78-320.jpg)
![[email_address] Slideshare.com](https://image.slidesharecdn.com/steve-vittos-assessing-and-treating-defiant-behavior-1209624284112203-8/85/Steve-Vittos-Assessing-And-Treating-Defiant-Behavior-92-320.jpg)

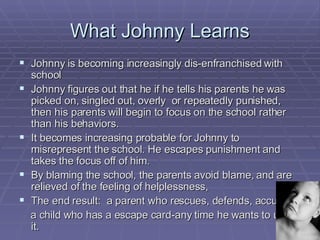
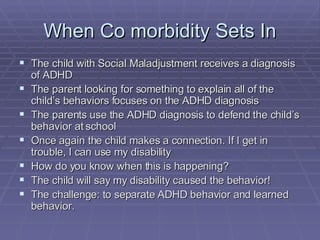
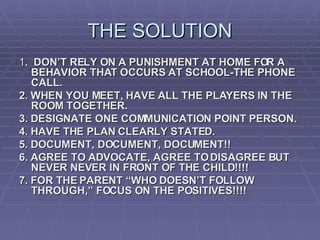
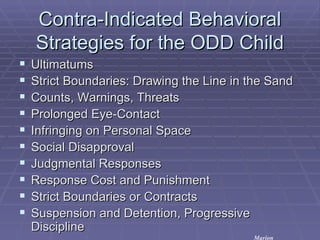
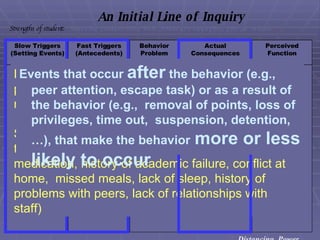
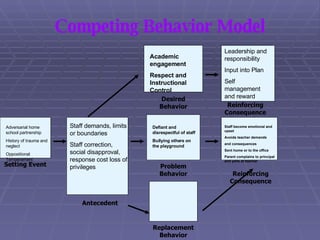
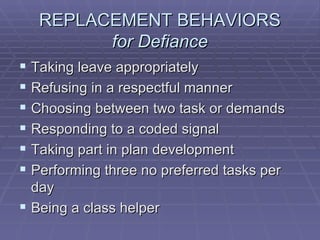
The document discusses assessment and treatment of defiant behavior in children using positive approaches. It notes that without evidence-based decision making, reliance on punishment can damage relationships between schools and parents and teach children to blame others. The document recommends focusing on communication, documentation, and agreeing to disagree respectfully to build partnerships in addressing problematic behaviors.






































































































