2
HOUSE RULES
1. Cometo class on time, in the right uniform, and well-
groomed.
2. Extend courtesy not only to the Professor but to everyone
as well. Act like future Professional Nurses.
3. Listen attentively, take down notes, and PARTICIPATE
ACTIVELY.
5. Three tardiness is equivalent to one day absent from class.
3.
HEALTH ASSESSMENT
• Thecourse deals with concepts, principles &
techniques of history taking using various
tools, physical examination (head to toe),
psychosocial assessment and interpretation
of laboratory findings to arrive at a nursing
diagnosis on the client across the lifespan in
community and hospital settings.
4.
4
TERMINAL COMPETENCIES
At theend of the course (36 hours) and given
simulated and actual conditions/ situations, the
student will be able to:
• Differentiate normal from abnormal assessment
findings;
• Utilize concepts, principles, techniques and
appropriate assessment tools in the assessment of
individual client with varying age group and
development;
• Observe bioethical concepts/ principles and core
values and nursing standards in the care of clients.
5.
Health Assessment inNursing
- Gathering of information about patient’s
PHYSIOLOGICAL, PSCHOLOGICAL SOCIAL
and SPIRITUAL status
- Critical investigation and evaluation of health
status
6.
TWO ASPECTS OFHEALTH ASSESSMENT
1. Nursing Health History
(SUBJECTIVE DATA)
2. Physical Examination
(OBJECTIVE DATA)
7.
STEPS OF HEALTHASSESSMENT:
The assessment phase of the nursing
process has four major steps:
1.Collection of subjective data
2.Collection of objective data
3. Validation of data
4. Documentation of data
8.
NURSING PROCESS
•Sets ofactions used to determine, plan,
implement and evaluate nursing care.
•Systematic, rational method of planning and
providing individualized care.
9.
PURPOSE
• To helpthe nurse manage each patient’s
nursing care, intelligently, scientifically and
judiciously.
• To identify a client’s health care status,and
actual or potential health problems, to
establish plans to meet the identified needs
and to deliver specific nursing interventions
to address those needs
10.
CHARACTERISTICS
• It iscyclical
• It is client centered
• It is problem solving-oriented
• It is goal-oriented
• Decision making is involved in every phase
• It is interpersonal and collaborative
• It is orderly and planned, step-by-step
• It is universally applicable to all patients,
families, and communities that nursing serves
11.
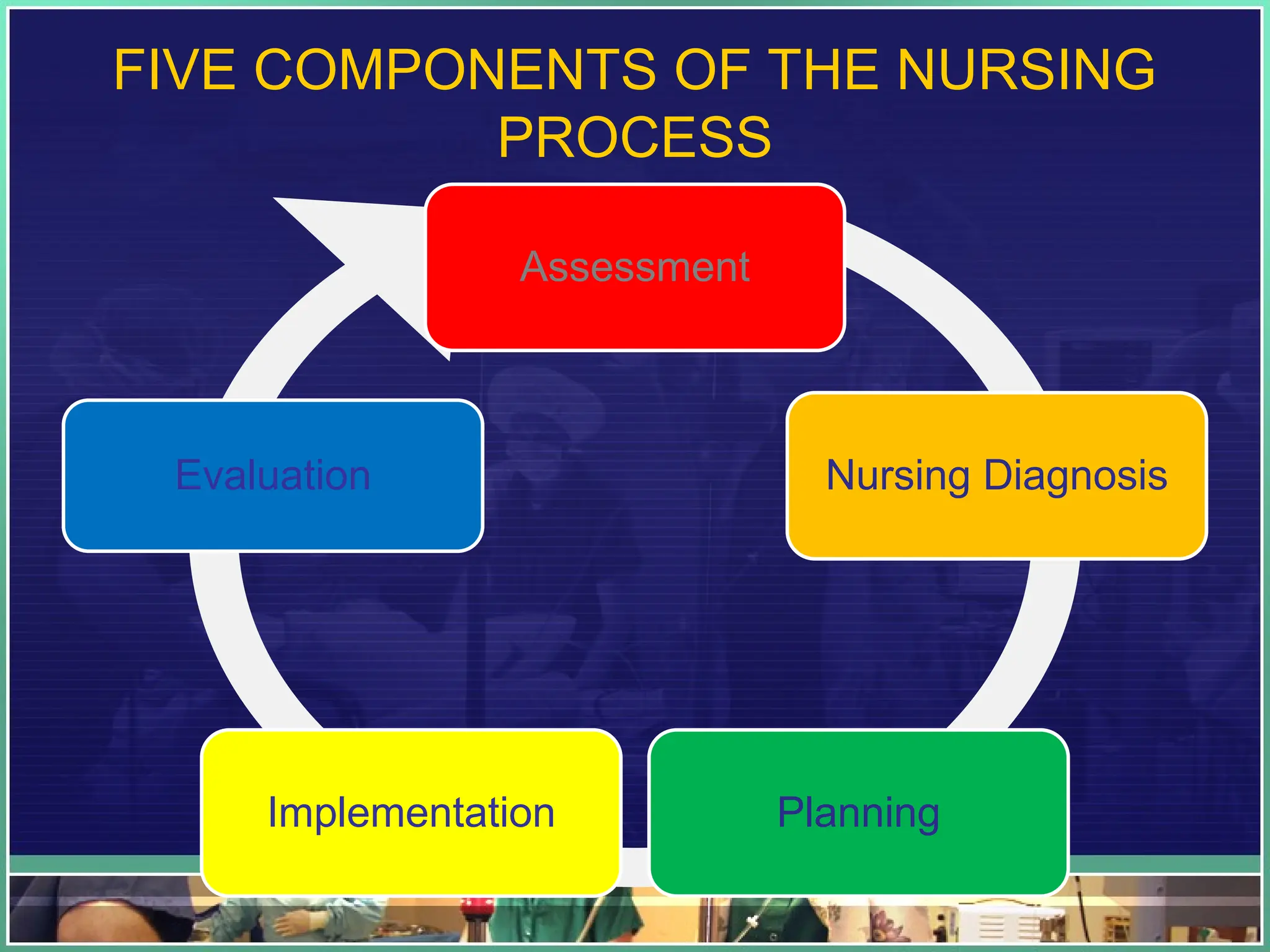
FIVE COMPONENTS OFTHE NURSING
PROCESS
Assessment
Nursing Diagnosis
Planning
Implementation
Evaluation
12.
12
Overview of theNursing Process
• Assessing- collecting, organizing, validating, and
documenting client data.
• Diagnosing- analyzing and synthesizing data
• Planning- determining how to prevent, reduce, or
resolve the identified priority client problems.
• Implementing- carrying out (or delegating) and
documenting the planned nursing interventions.
• Evaluating- measuring the degree to which goals/
outcomes have been achieved.
13.
Nursing Process inAction
•Assessing
•- collect data, organize data, validate data, document
data
•Diagnosing
•- analyze data, identify health problems, risks and
strengths, formulate diagnostic statements
•Planning
•Prioritize problems/diagnoses, formulate
goals/desired outcomes, select nursing interventions,
write nursing interventions
14.
• Implementing
• Reassessthe client, determine the nurse’s need for
assistance, implement the nursing interventions,
supervise delegated care, document nursing
activities
• Evaluating
• Collect data related to outcomes, compare data
with outcomes, relate nursing actions to client
goals/outcomes, draw conclusions about problem
status, continue, modify, or terminate the client’s
care plan.
15.
Assessment: The FirstPhase of the
Nursing Process
• the most critical phase of the nursing process
• deliberate and systematic collection of data to
determine client’s current and past health and
functional status.
• determines client’s current and past coping
patterns
16.
Assessment: The FirstPhase of the
Nursing Process
• is ongoing and continuous throughout all the
phases of the nursing process.
• The purpose of a nursing health assessment is to
collect holistic subjective and objective data to determine
a client’s overall level of functioning in order to make a
professional clinical judgment.
• The nurse collects physiologic, psychological,
sociocultural, developmental, and spiritual data about the
client. Thus the nurse performs holistic data collection
17.
A Critical ThinkingApproach to Assessment
• Analysis
• Analysis
• Analysis
• Analysis
Client’s
Record
Client
Client’s
Significant
others
Health Team
Members
18.
18
Subjective & ObjectiveData
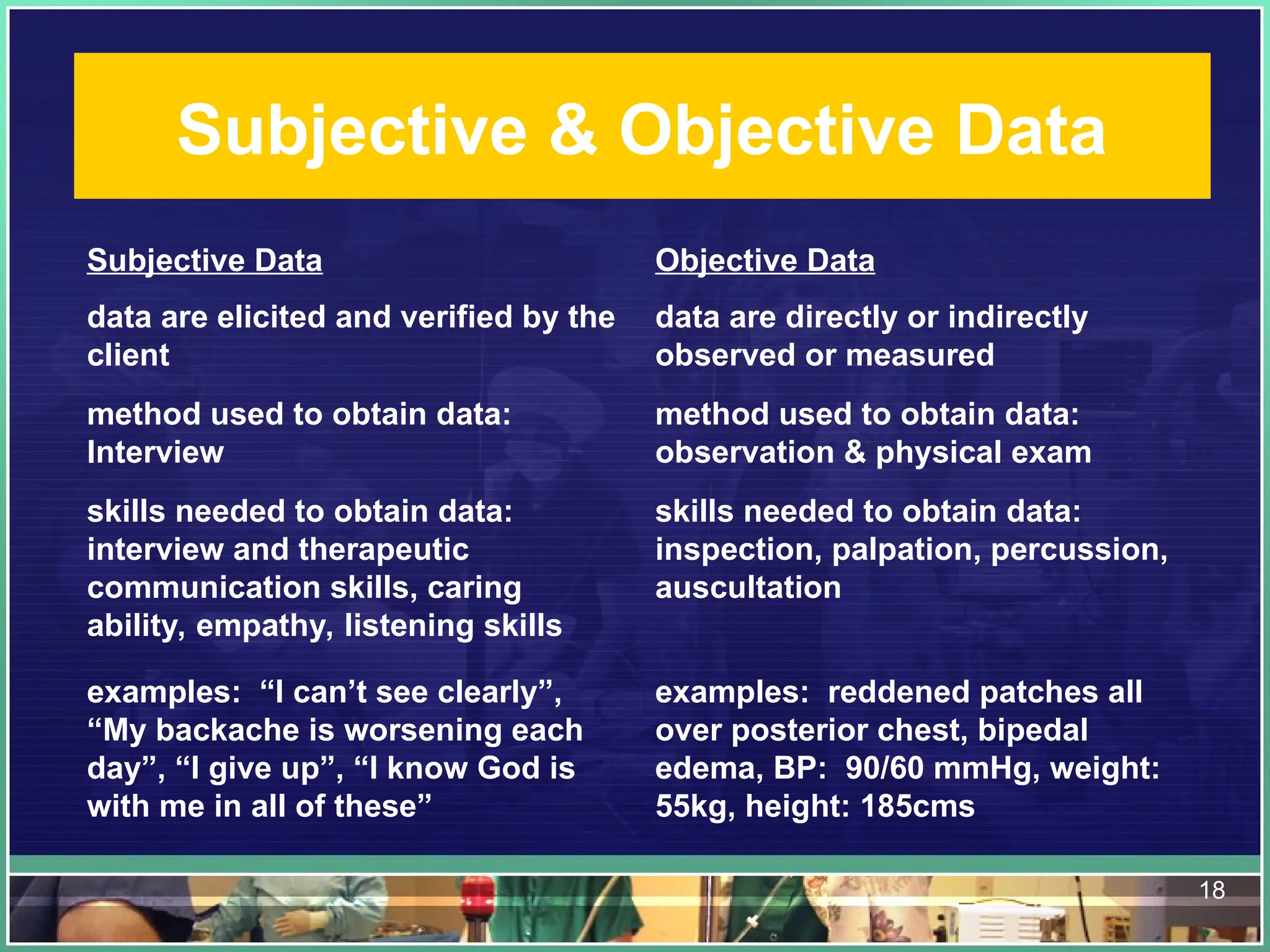
Subjective Data Objective Data
data are elicited and verified by the
client
data are directly or indirectly
observed or measured
method used to obtain data:
Interview
method used to obtain data:
observation & physical exam
skills needed to obtain data:
interview and therapeutic
communication skills, caring
ability, empathy, listening skills
skills needed to obtain data:
inspection, palpation, percussion,
auscultation
examples: “I can’t see clearly”,
“My backache is worsening each
day”, “I give up”, “I know God is
with me in all of these”
examples: reddened patches all
over posterior chest, bipedal
edema, BP: 90/60 mmHg, weight:
55kg, height: 185cms
19.
• Subjective dataare sensations or symptoms (e.g., pain,
hunger), feelings (e.g., happiness, sadness), perceptions,
desires, preferences, beliefs, ideas, values, and personal
information that can be elicited and verified only by the
client.
• Objective data-
• obtained by general observation and by using the four physical
examination techniques: inspection, palpation, percussion, and
auscultation. Another source of objective data is the client’s
medical/health record, which is the document that contains information
about what other health care professionals
• Physical characteristics (e.g., skin color, posture) • Body functions (e.g.,
heart rate, respiratory rate) • Appearance (e.g., dress and hygiene) • Behavior
(e.g., mood, affect) • Measurements (e.g., blood pressure, temperature, height,
weight) • Results of laboratory testing (e.g., platelet count, x-ray findings)
20.
TYPES OF HEALTHASSESSMENT:
The four basic types of assessment are:
1.Initial comprehensive assessment
2,Ongoing or partial assessment
3. Focused or problem-oriented assessment
4. Emergency assessment
21.
1. Initial comprehensiveassessment
involves collection of subjective data about the client’s perception of his or her health of
all body parts or systems, past health history, family history, and lifestyle and health
practices (which includes information related to the client’s overall function) as well
as objective data gathered during a step-by-step physical examination.
- is needed when the client first enters a health care system and periodically thereafter
to establish baseline data against which future health status changes can be
measured and compared.
-Example: Assessment upon admission of the patient
2. Ongoing or Partial Assessment
- This consists of a mini-overview of the client’s body systems and holistic health
patterns as a follow-up on health status. Any problems that were initially detected in
the client’s body system or holistic health patterns are reassessed to determine any
changes.
- For example, a client admitted to the hospital with lung cancer requires frequent
assessment of lung sounds.
22.
• 3. Focusedor Problem-Oriented Assessment
• - It is performed when a comprehensive database exists for a client who
comes to the health care agency with a specific health concern
• - For example, if your client tells you that he has pain you would ask him
questions about the character and location of pain, onset, relieving and
aggravating factors, and associated symptoms.
• 4. Emergency Assessment
• - An emergency assessment is a very rapid assessment performed in
life-threatening situation
• -An example of an emergency assessment is the evaluation of the
client’s airway, breathing, and circulation (known as the ABCs) when
cardiac arrest is suspected. The major and only concern during this type
of assessment is to determine the status of the client’s lifesustaining
physical functions.
23.
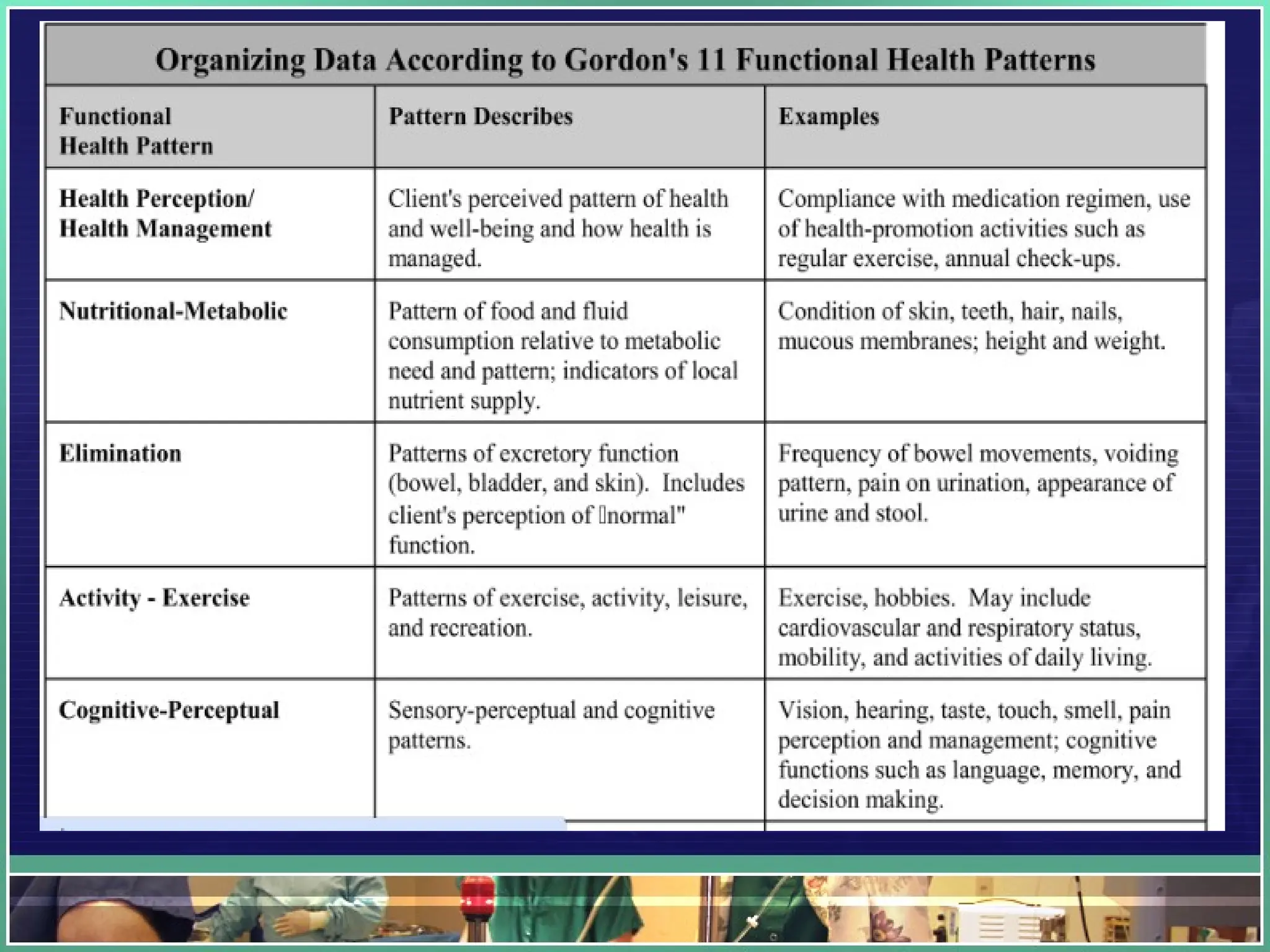
Gordon's Functional HealthPatterns
Gordon’s functional health patterns is a method devised by Marjory Gordon to be
used by nurses in the nursing process to provide a more comprehensive
nursing assessment of the patient.
The following areas are assessed through questions asked by the nurse and
medical examinations to provide an overview of the individual's health status and
health practices that are used to reach the current level of health or wellness
24.
• Marjorie Gordon(1987) proposed functional
health patterns as a guide for establishing a
comprehensive nursing data base.
• These 11 categories make possible a
systematic and standardized approach to
data collection, and enable the nurse to
determine the following aspects of health and
human function
25.
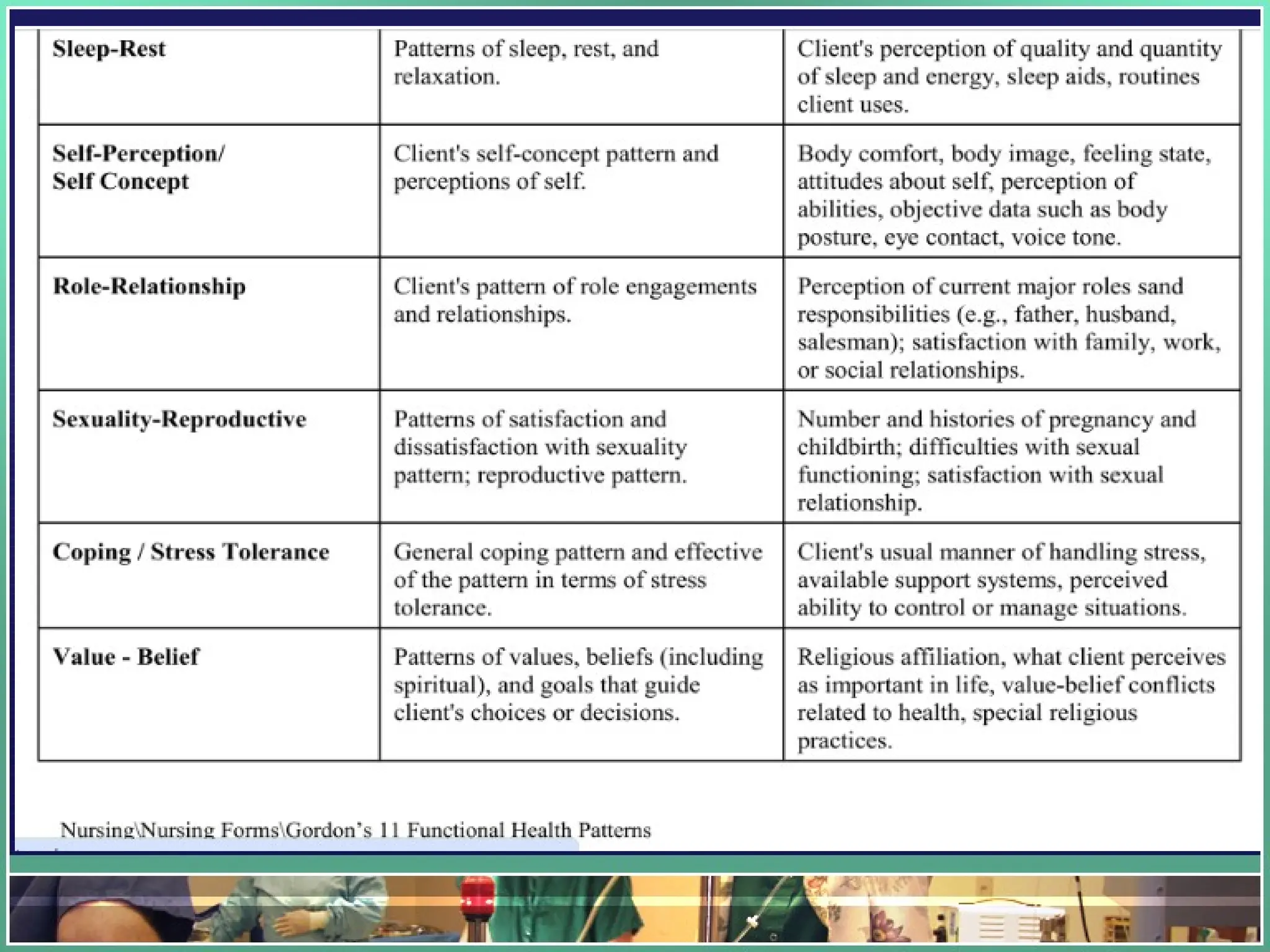
Gordon's 11 FunctionalHealth
Patterns
1. Health Perception and Health Management.
2. Nutrition and Metabolism
3. Elimination
4. Activity and Exercise.
5. Cognition and Perception.
6. Sleep and Rest.
7. Self-Perception and Self-Concept.
8. Roles and Relationships.
9. Sexuality and Reproduction.
10. Coping and Stress Tolerance.
11. Values and Belief.
8 Sections ofa Complete Health History
• Biographic data
• Reasons for seeking health care (Chief Complaint)
• History of present health concern
• Past health history
• Family health history
• Review of systems for current health problems
• Lifestyle and practices profile
• Developmental level (Objective Data)
30.
8 Sections ofa Complete Health History
• Biographic data
• Reasons for seeking health care (Chief Complaint)
• History of present health concern
• Past health history
• Family health history
• Review of systems for current health problems
• Lifestyle and practices profile
• Developmental level
31.
BIOGRAPHIC DATA
• Includesinformation that identifies the client
– E.g. name, address, phone number, gender etc.
– Source of data:
• Client or significant others
32.
REASON(S) FOR SEEKINGHEALTH CARE
• Also known as Client’s Chief Complaint (CC)
• We aim to determine the following:
– What brought the client to seek health care
– The feelings of the client about seeking health care
• Can be assessed by asking the following questions:
– “What is your major health problem or concerns at this time?”
– "How do you feel about having seeking health care?”
33.
“What is yourmajor health problem or
concerns at this time?”
• Assist the client to focus on his most significant concern
• Other questions like, “ Why are you here?” and “How
can I help you?” can also be asked
– Reminder: use holistic approach in phrasing questions,
draw out concerns that are beyond just a physical
complaint and address other associated factors like
stress or lifestyle changes
34.
"How do youfeel about having seeking
health care?”
• Encourages the client to discuss fears or feelings
about having to seek health care advice.
• May help in determining descriptions of past
experiences—both positive and negative—with
other health care worker
35.
HISTORY OF PRESENTHEALTH CONCERN
• takes into account several aspects of client’s
current health concern
• includes questions that provide detailed
descriptions of the client’s health problem
36.
Encourage the clientto explain:
• health problem or symptom focusing on onset, progression
and duration
• signs and symptoms and related problems
• what the client perceives as causing the problem/symptom
• what makes the problem worse
• what makes the problem better
• which treatments have been tried
• what effect the problem has had on daily life
• what is the client’s ability to provide self-care
37.
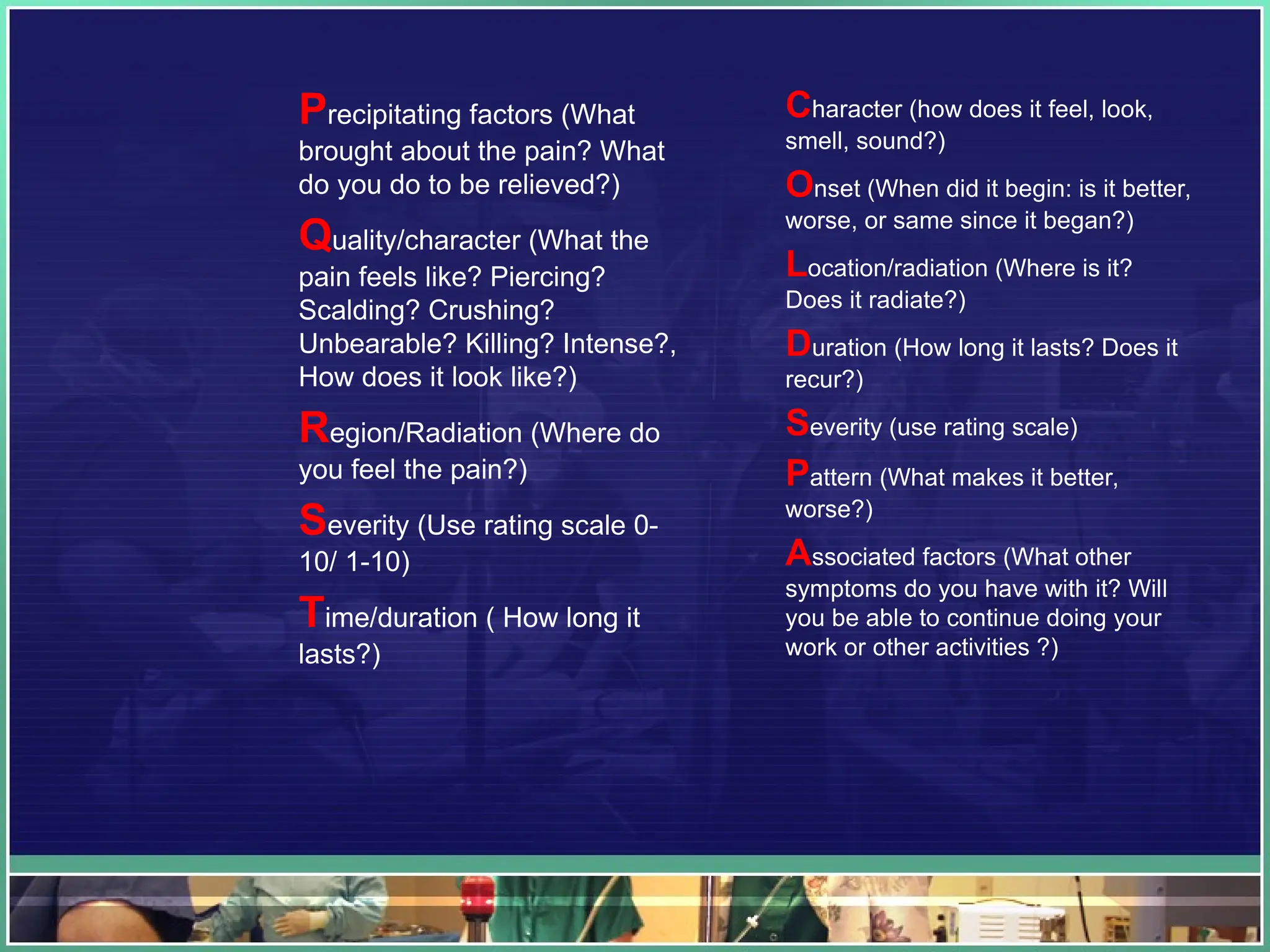
TIP: USE MNEMONICS
•To gather a comprehensive history of present concern as a nurse
you may use the following mnemonic to organize data:
• PQRST or COLDSPA
38.
Precipitating factors (What
broughtabout the pain? What
do you do to be relieved?)
Quality/character (What the
pain feels like? Piercing?
Scalding? Crushing?
Unbearable? Killing? Intense?,
How does it look like?)
Region/Radiation (Where do
you feel the pain?)
Severity (Use rating scale 0-
10/ 1-10)
Time/duration ( How long it
lasts?)
Character (how does it feel, look,
smell, sound?)
Onset (When did it begin: is it better,
worse, or same since it began?)
Location/radiation (Where is it?
Does it radiate?)
Duration (How long it lasts? Does it
recur?)
Severity (use rating scale)
Pattern (What makes it better,
worse?)
Associated factors (What other
symptoms do you have with it? Will
you be able to continue doing your
work or other activities ?)
39.
PAST HEALTH HISTORY
•elicit data related to the client’s strengths and
weaknesses in his health history
– Physical, social, emotional or spiritual
• may also include trends of unhealthy
behaviors
– Vices or lack of physical activity
• data obtained in this section aids the nurse
to identify risk factors that stem from
previous health problems (risk factors may
be to the client or significant others)
40.
Past Health History
includesquestions about...
• birth, growth and development
• childhood diseases
• immunizations
• allergies
• previous health problems
• hospitalizations and surgeries
• pregnancies
• births
• previous accidents and injuries
• pain experiences
• emotional or psychological problems
41.
FAMILY HEALTH HISTORY
•focuses on health problems that seem to
run in families or those that are genetically
based
• should include as many genetic relatives as
the client can recall
• include maternal and paternal grandparents,
aunts and uncles on both sides, parents,
siblings and the client’s children
42.
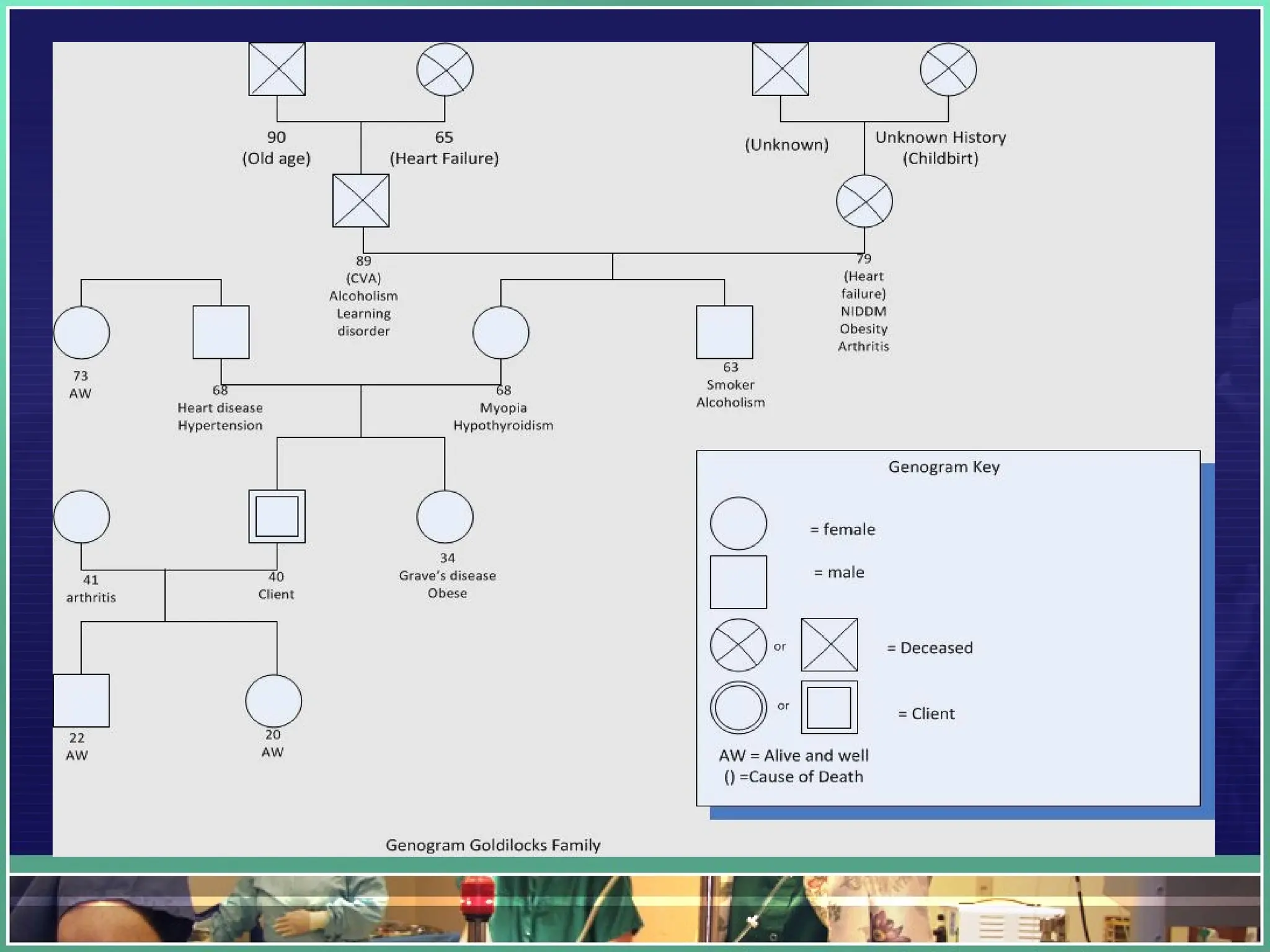
FAMILY HEALTH HISTORY
•drawing a Genogram helps to organize and illustrate the client’s
family history
• use a standard format
• provide a key for the entries
– female relatives: circle
– male relatives: square
– deceased relative: marking an X in the circle or square and listing the age
at death
– cause of death noted inside a parenthesis e.g. (heart failure )
– AW (Alive and well) should be placed next to the age
– Straight or vertical lines to denote relationship
– Horizontal doted line to indicate client’s spouse
– Vertical dotted line to indicate adoption
44.
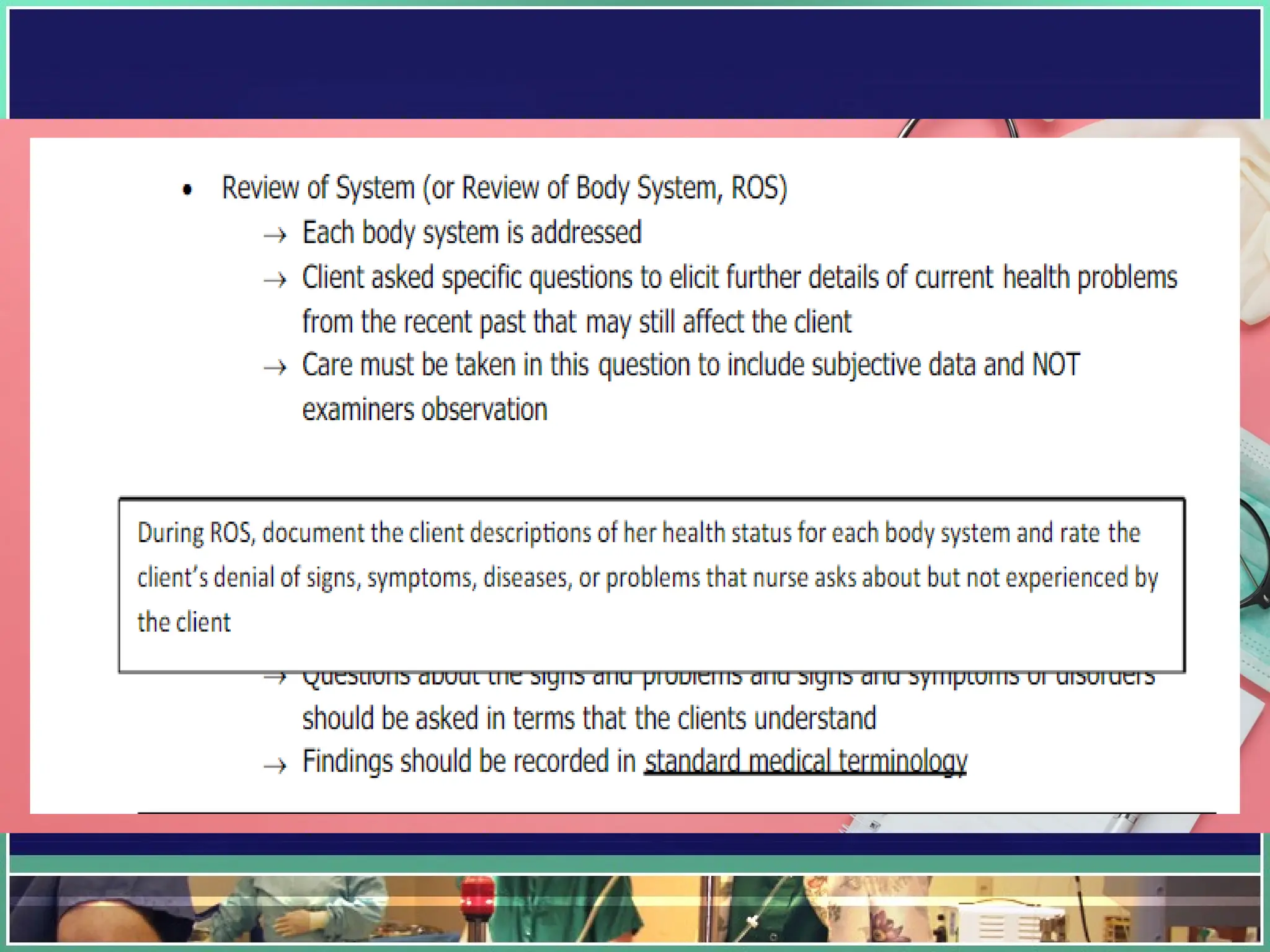
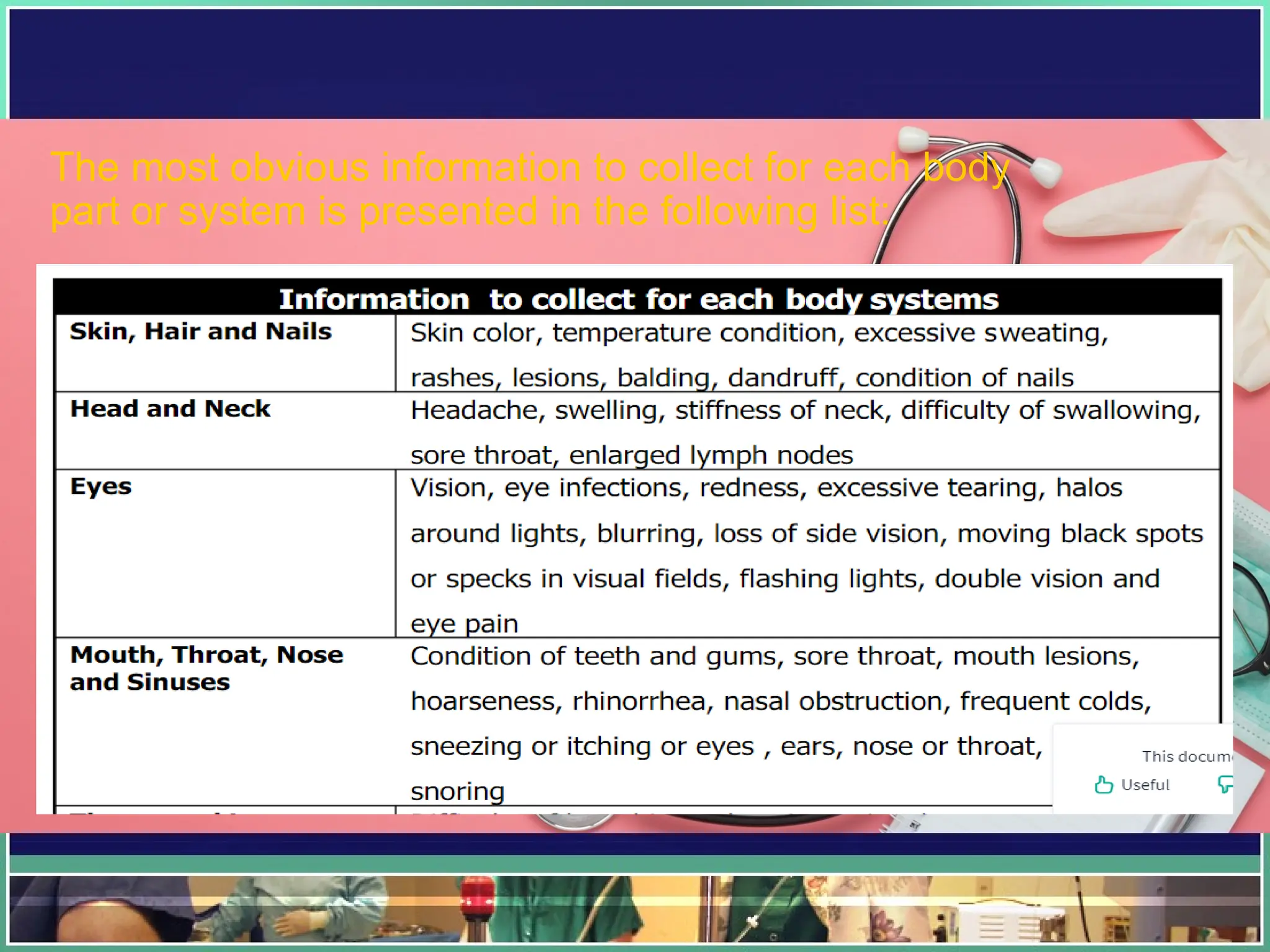
REVIEW OF SYSTEMS
(ROS)FOR CURRENT
HEALTH PROBLEM
In here, each body system is addressed, and
the client is asked specific questions to draw
out current health problems or problems from
the recent past that may still affect the client or
that are recurring.
During the review of body systems, document
the clients descriptions of her health status for
each body system and note the client’s denial
of signs and symptoms, diseases or problems
that the nurse ask about but are not
experienced by the client
46.
The most obviousinformation to collect for each body
part or system is presented in the following list:
47.
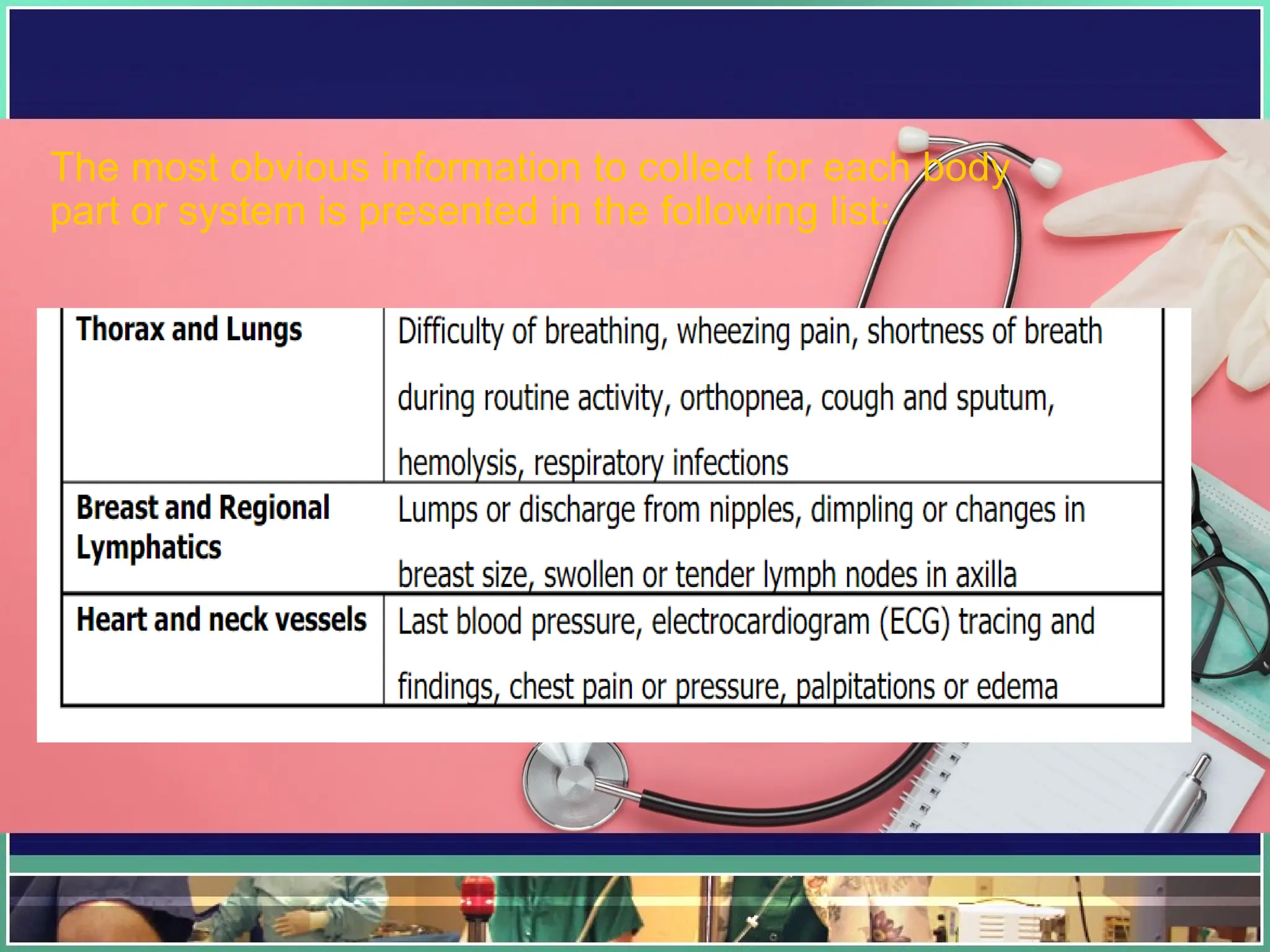
The most obviousinformation to collect for each body
part or system is presented in the following list:
48.
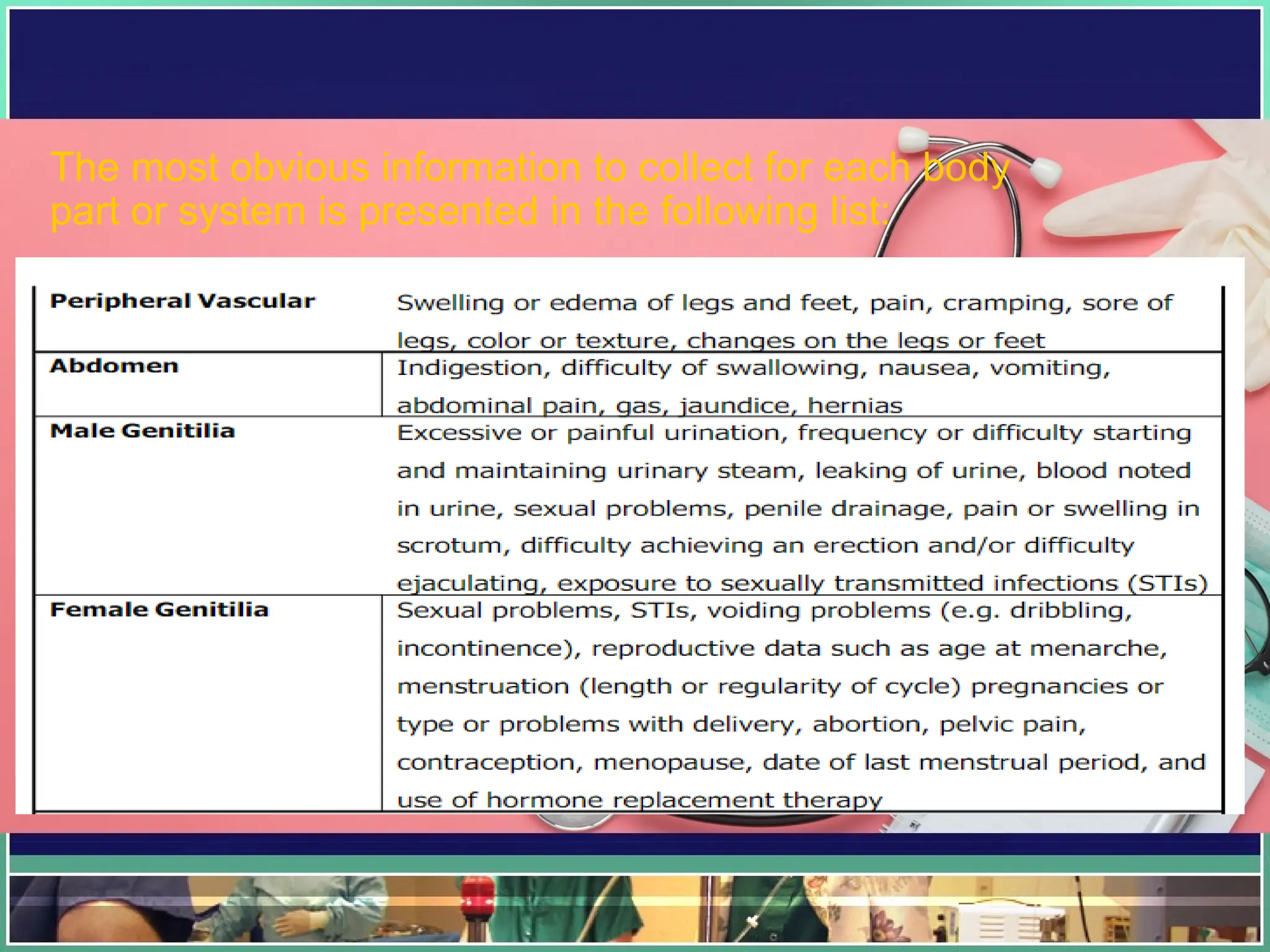
The most obviousinformation to collect for each body
part or system is presented in the following list:
49.
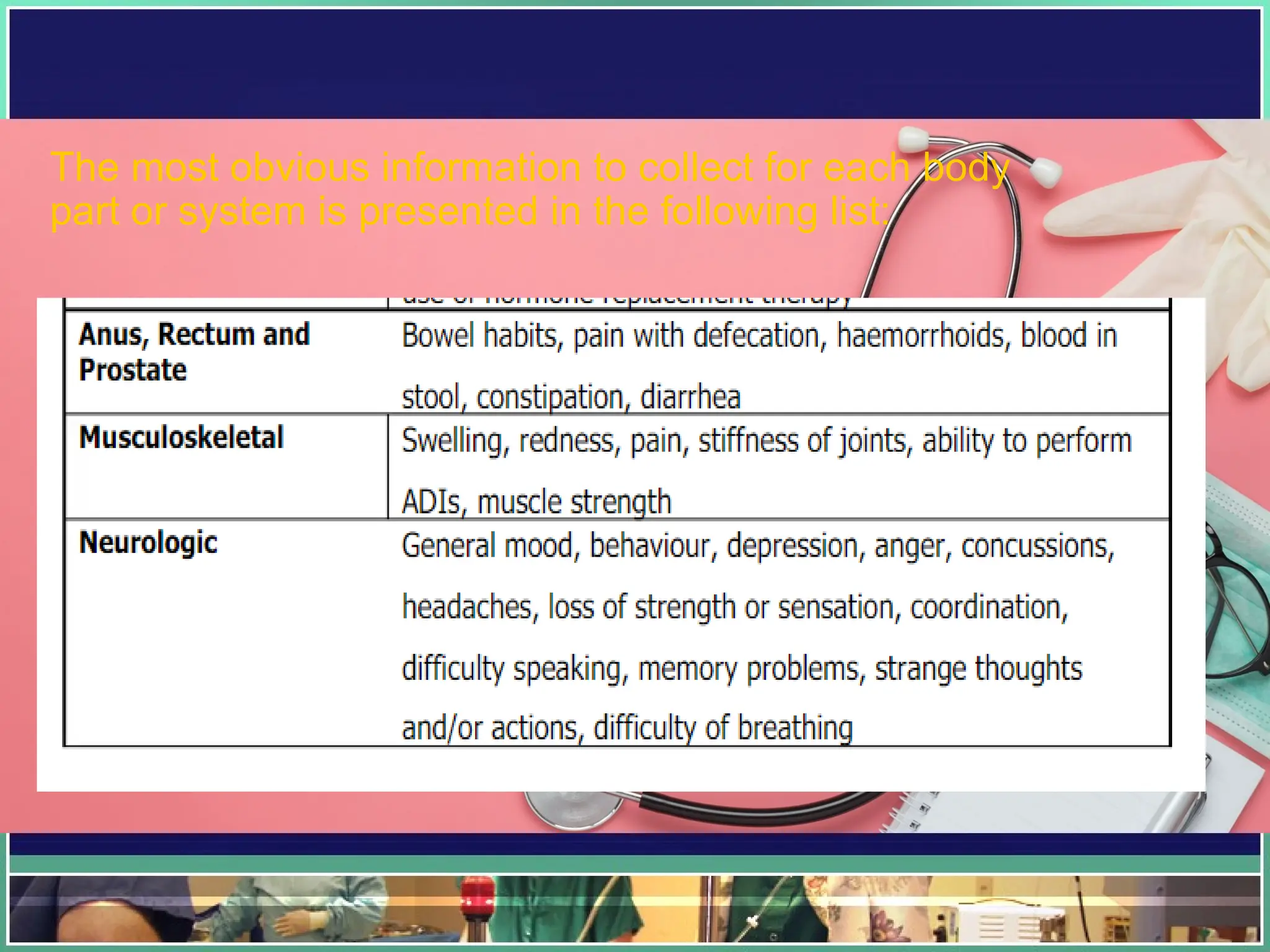
The most obviousinformation to collect for each body
part or system is presented in the following list:
50.
LIFESTYLE AND HEALTH
PRACTICESPROFILE
This is a very important section of the health
history because it deals with the client’s human
responses, which include:
• nutritional habits,
• activity and exercise patterns,
• sleep and rest patterns,
• self-concept and self-care activities,
•social and community activities,
•relationships,
• values and beliefs system,
•education and work,
•stress level and coping style, and
• environment
51.
DEVELOPMENTAL
LEVEL
FREUD’S THEORYOF
PSYCHOSEXUAL DEVELOPMENT
ERIKSON’S THEORY OF
PSYCHOSOCIAL DEVELOPMEN
PIAGET’S THEORY OF COGNITIVE
DEVELOPMENT
KOHLBERG’S THEORY OF MORAL
DEVELOPMENT
53.
Functional Assessment ofNewborns,
Infants & Children, Adults/Elderly
• Newborn (APGAR Scoring & anthropometric
measurements)
• Infants & Children (MMDST & some major
developmental milestones)
• Adults/Elderly (PADC, Lawton Scale for IADL,
KATZ index of independence on ADL, Barthel
Index)
54.
This scoring systemis a method of
measuring a baby’s vitals and overall health
shortly after childbirth
A stands for Appearance (skin color)
P stands for Pulse (heart rate)
G stands for Grimace response (reflexes)
A stands for Activity (muscle tone)
R stands for Respiration (breathing rate and
effort)
55.
Initial Newborn Assessment...Apgar
Scoring
•provides numeric indicator of newborn’s physiologic
capacity to adapt to extra-uterine life
• assessed at 1 and at 5 minutes after delivery
• each of the five aspects is assigned a maximum score
of 2
• maximum achievable total score is 10
• score under 7 suggests that the baby is having difficulty
• score under 4 indicates that the baby’s condition is
critical
• those with very low scores require special resuscitative
measures and care
56.
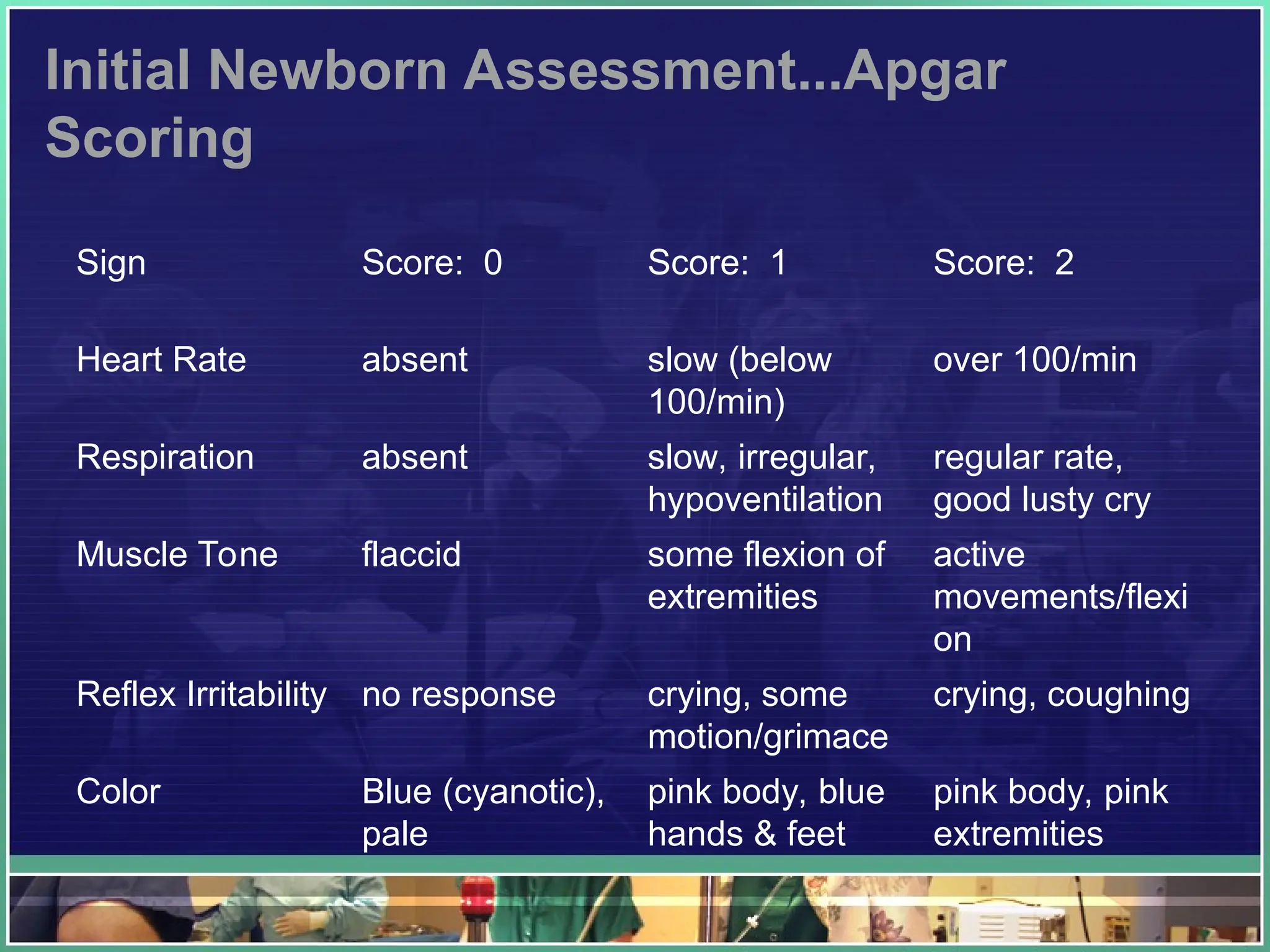
Initial Newborn Assessment...Apgar
Scoring
SignScore: 0 Score: 1 Score: 2
Heart Rate absent slow (below
100/min)
over 100/min
Respiration absent slow, irregular,
hypoventilation
regular rate,
good lusty cry
Muscle Tone flaccid some flexion of
extremities
active
movements/flexi
on
Reflex Irritability no response crying, some
motion/grimace
crying, coughing
Color Blue (cyanotic),
pale
pink body, blue
hands & feet
pink body, pink
extremities
Newborn’s Anthropometric
Measurements...weight
• atbirth most babies weigh from 2.7 to 3.8 kg (Kozier et
al)...2500 to 4000 g (Weber & Kelly)
• just after birth, newborns lose 5% to 10% of their birth
weight because of fluid loss (normal)
• regains birth weight in about 1 week
• at 5 to 6 months, infants usually reach twice their birth
weight
• by age 12 months, infants weight is usually 3 times their
birth weight
• weigh the newborn unclothed using a newborn scale
59.
59
Newborn’s Anthropometric
Measurements...length
• averagelength varies
• female babies are usually smaller in length than
male babies
• rate of increase in height/length is largely
influenced by the baby’s size at birth and by
nutrition
• measure the newborn from head-to-heel (from
the top of the head to the base of the heels)
60.
Newborn’s Anthropometric
Measurements...head &chest
circumference
• normal head circumference (normocephaly) should be assessed in
relation to chest circumference
• chest circumference of the newborn is usually less than the head
circumference by about 2.5 cm (1 in)
• as the infant grows, chest circumference becomes larger than the
head circumference
• at about 9 or 10 months, head and chest circumferences are almost
the same
• after 1 year of age, chest circumference is larger
• a newborn’s head circumference is measured around the skull
above the eyebrows
• measure chest circumference by placing tape measure at nipple line
and wrap it around the newborn
Developmental Assessment ofInfants
and Children...MMDST
• adopted from Denver Developmental Screening
Test (DDST)
• a screening tool to identify developmental delays
among children from birth to 6 years of age
• intended to estimate the abilities of a child
compared to those of an average group of
children of the same age
• not a test of intelligence
63.
Developmental Assessment ofInfants
and Children...MMDST
•four main areas of development are screened:
1. personal-social
2. fine-motor adaptive
3. language
4. gross motor
64.
Developmental Assessment ofInfants and
Children...MMDST
• personal-social – tasks which indicate the child’s
ability to get along with people and to take care of
himself
• fine motor adaptive – tasks which indicate the
child’s ability to see and use his hands to pick up
objects and to draw
• Language – tasks which indicate the child’s ability
to hear, follow directions and to speak
• Gross motor – tasks which indicate the child’s
ability to sit, walk and jump
65.
Assessment of aPregnant
Woman...Estimating Delivery Date
• Nagel’s Rule: subtract 3 months from the first day
of the last menstrual period (LMP) and add 7 days.
Ex: LMP= Oct. 5, 2010
Oct. 5 – 3months= July 3(because Aug. & July have
31 days) thus,
EDD= July 3+7days=July 10, 2011
66.
Assessment of aPregnant
Woman...Estimating Age of Gestation
• through LMP
• using McDonald’s Rule
fundal height in cm x 2/7 = AOG in months
fundal height in cm x 8/7 = AOG in weeks
67.
Assessment of aPregnant
Woman...Maternal History
• age
• family history
• pregnant woman’s medical history
• pregnant woman’s past obstetric history
• pregnant woman’s present obstetric history
68.
Assessment of aPregnant
Woman...Maternal History
• age as a risk factor: very young; older women
• family history: congenital disorders, multiple
pregnancies, DM, heart disease, hypertension,
mental retardation
• woman’s medical history: menarche, childhood
diseases, major illnesses, surgery, blood
transfusion, drug sensitivity, urinary infections,
heart disease, diabetes, hypertension, endocrine
disorders, anemia, use of contraceptives, drug
abuse, alcohol and tobacco use
69.
Assessment of aPregnant Woman...Maternal
History
• past obstetric history – previous pregnancies
(gravida) and deliveries (parity), types of
deliveries, multiple births (multipara), abortions,
maternal, fetal and neoatal complications,
perceptions of past pregnancies, labor and
delivery
70.
Assessment of aPregnant
Woman...Maternal History
• present obstetric history
gravidity, parity
LMP
EDD
signs and symptoms of pregnancy
rest and sleep patterns
activity and employment, if any
sexual activity
diet history, eating pattern, weight loss, weight
gain
71.
Assessment of aPregnant
Woman...Maternal History
• psychosocial status – emotional changes client is
experiencing, reactions to the present pregnancy
(including her family’s response), support system
72.
Assessment of anElderly Client
• differentiate findings that result from the usual
“wear and tear”/degenerative processes and
those that indicate pathologic process
• “frail elderly”– vulnerability of aged people to be
in poorer health, to have more chronic
disabilities and to function less independently
73.
Assessment of anElderly Client
• symptoms of a disease may be more subtle in
advanced age
• changes in functional abilities may herald the
occurrence of a potential health problem
• recognizing changes in functional ability is often
crucial for prompt and accurate management of
both acute and chronic illness in an elderly
74.
Assessment of anElderly Client
• geriatric syndromes – the unique way in which a disease
presents in a frail elderly. These syndromes include:
• sleep disorders
• problems with eating or feeding
• incontinence (bladder and bowel)
• confusion
• evidence of falls
• skin breakdown
75.
Determining Functional Statusof an Elderly
• functional assessment – an evaluation of the
person’s ability to carry out the basic self-care
activities of daily living (ADLs) such as bathing,
eating, grooming and toileting
• functional assessment also includes those activities
necessary for well-being and survival as an
individual in a society (instrumental activities of
daily living
76.
Determining Functional Statusof an
Elderly
• Instrumental Activities of Daily Living (IADL) –
focus primarily on household chores, mobility-
related activities (ex. shopping and
transportation) and cognitive abilities (ex. money
management, making decisions affecting basic
safety and social needs) )...see display 30-8 on
page 820 of your book by Weber & Kelly
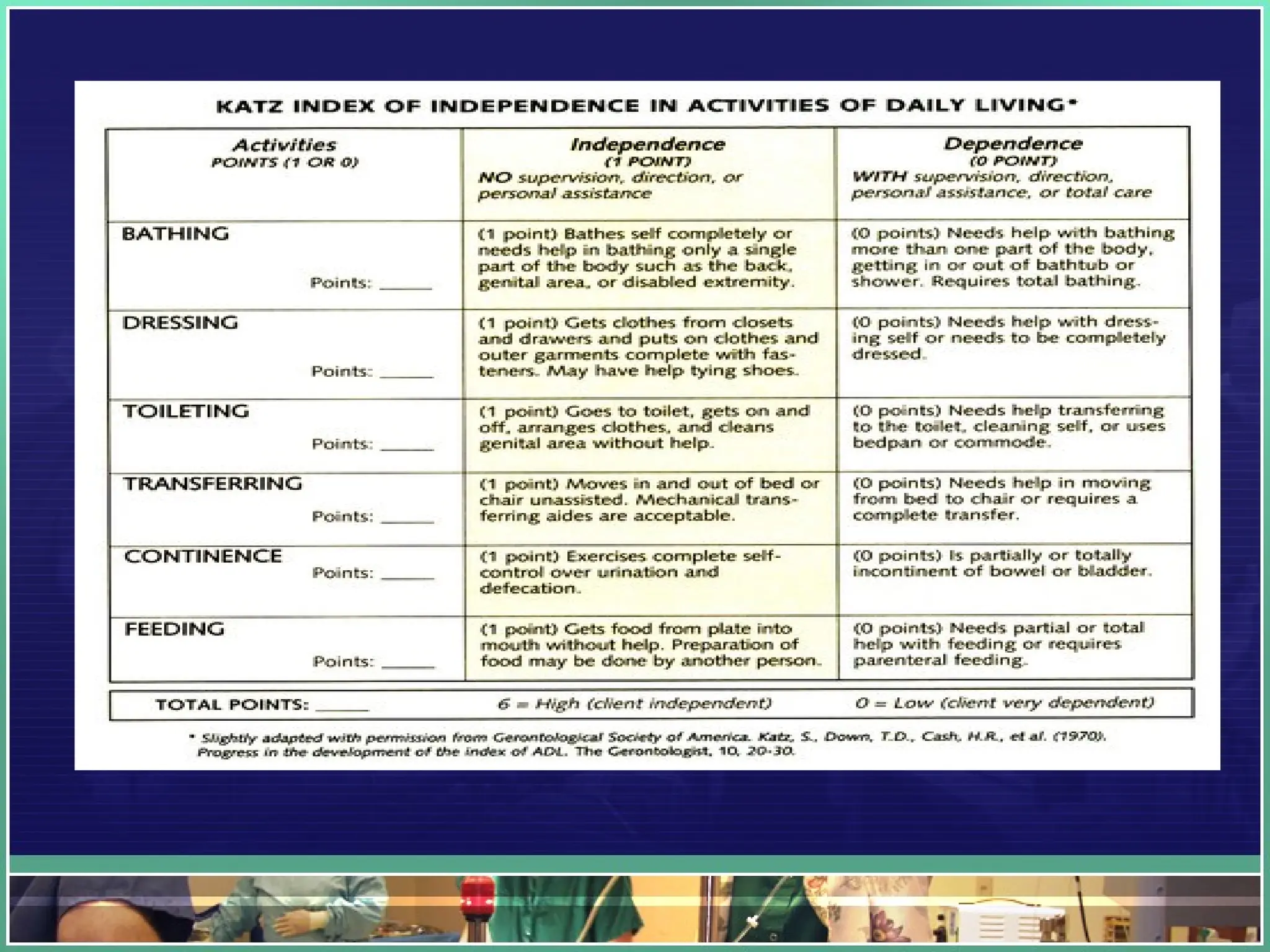
77.
Determining Functional Statusof an
Elderly
• Katz Activities of Daily Living – a commonly
used tool for measuring the ability to perform
basic personal tools such as bathing, dressing,
toileting, transferring and eating...see display 30-7
on page 819 of your book by Weber & Kelly
79.
Goal of ElderlyAssessment
• the ultimate goal of elderly assessment and
intervention should be to empower clients to
maintain the relationships, activities and events that
elderly clients find meaningful
• elderly assessment may not be focused on disease
prevention as it is on minimizing the disability
associated with chronic illness and preventing
complications and exacerbations of chronic
maladies
Editor's Notes
#58 details of the procedure will be dealt with in greater detail during NCM 101 and NCM 102