This document summarizes information about Staphylococci and Streptococci bacteria. It discusses their microscopic morphology, cultivation characteristics, biochemical features, virulence factors, clinical presentations, and treatment. Key points include:
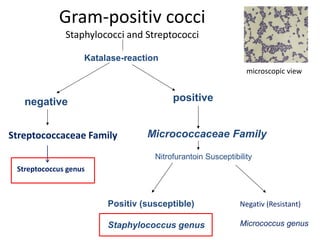
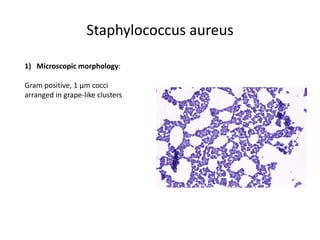
- Staphylococci are Gram-positive cocci that can be coagulase-positive like S. aureus or coagulase-negative like S. epidermidis. S. aureus is an important human pathogen able to cause both localized and invasive infections.
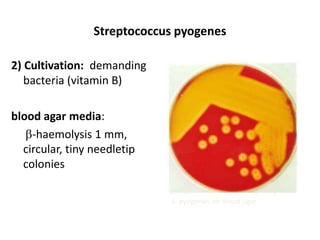
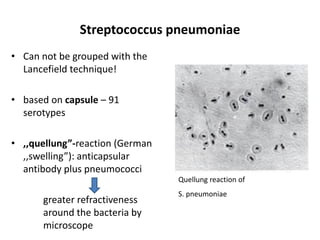
- Streptococci are Gram-positive cocci arranged in chains. Important species include S. pyogenes (Group A Strep) which causes pharyngitis and can lead to post-stre