

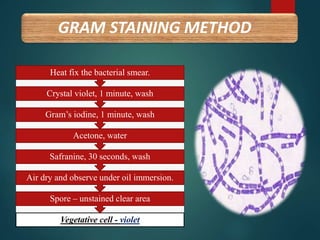
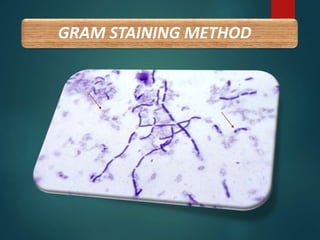
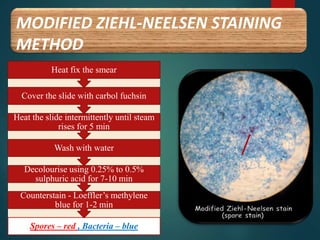
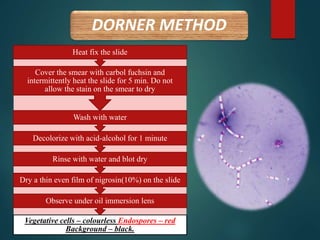
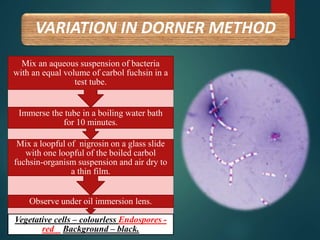
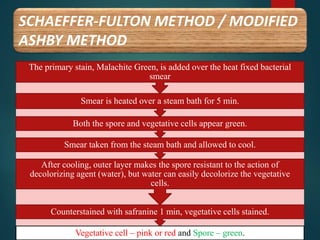
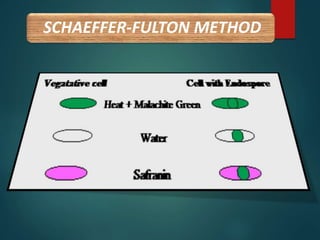
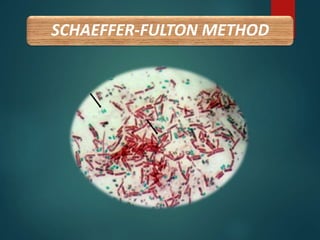
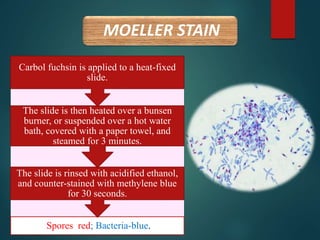
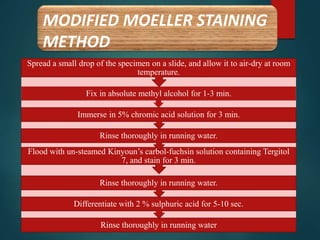
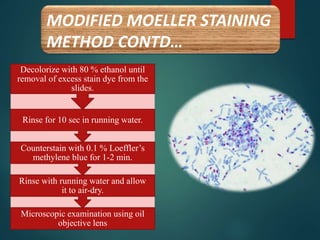
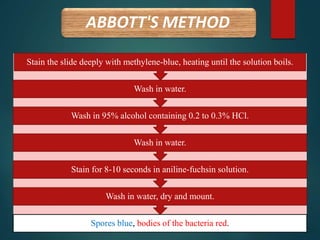
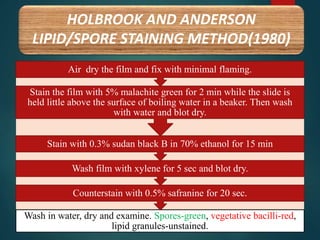
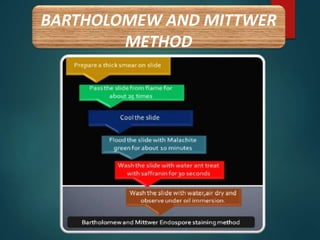



The document discusses various methods for staining bacterial endospores, including Gram staining, modified Ziehl-Neelsen staining, Dorner's method, Schaeffer-Fulton method, Moeller staining, and Abbott's method. Each method uses different primary and counter stains to differentially stain the endospores and vegetative cells. The document provides details on the staining procedures and reagents used for each method as well as the expected color results, with endospores typically staining red or green and vegetative cells staining blue, violet or colorless.



































































