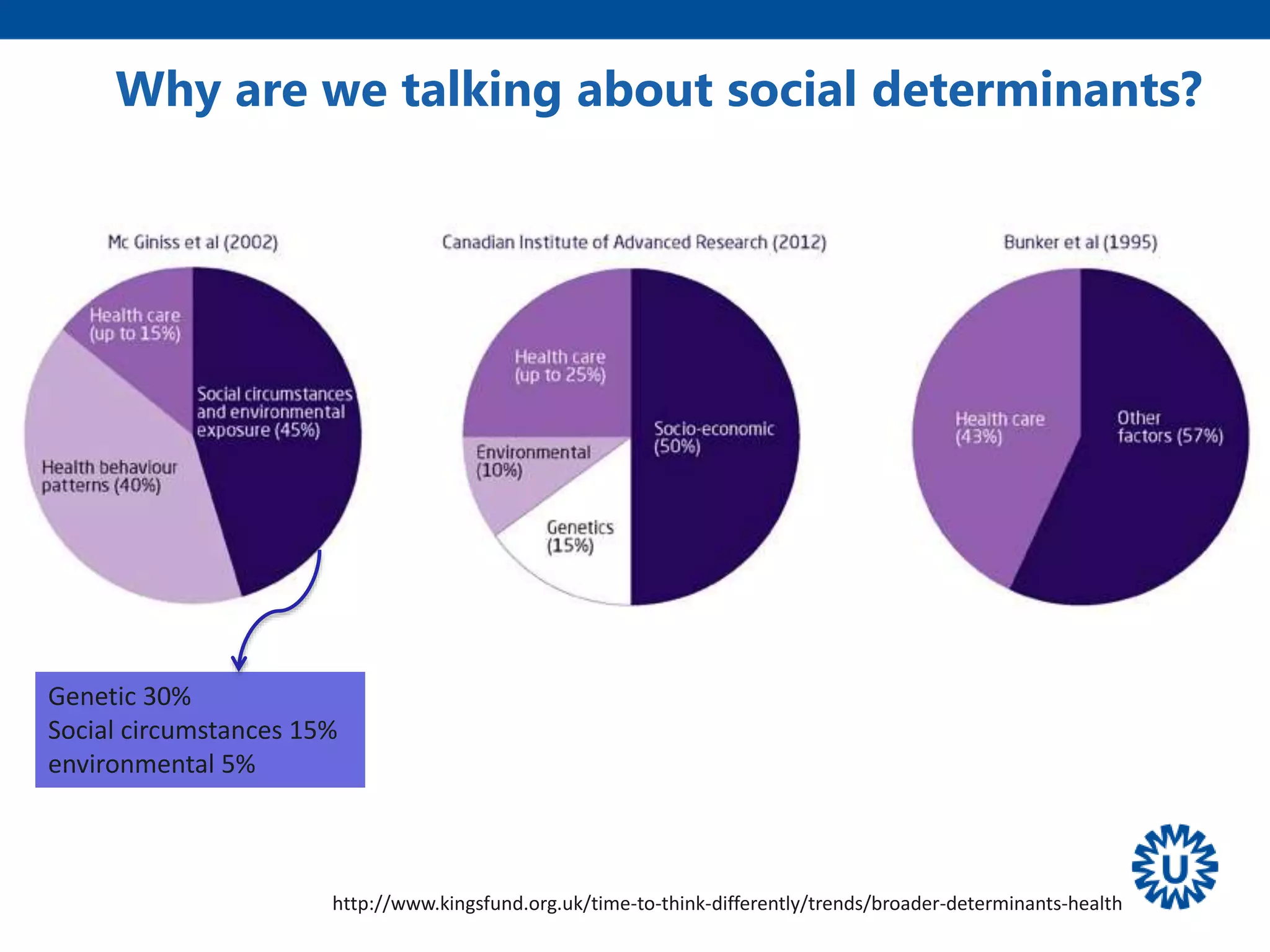
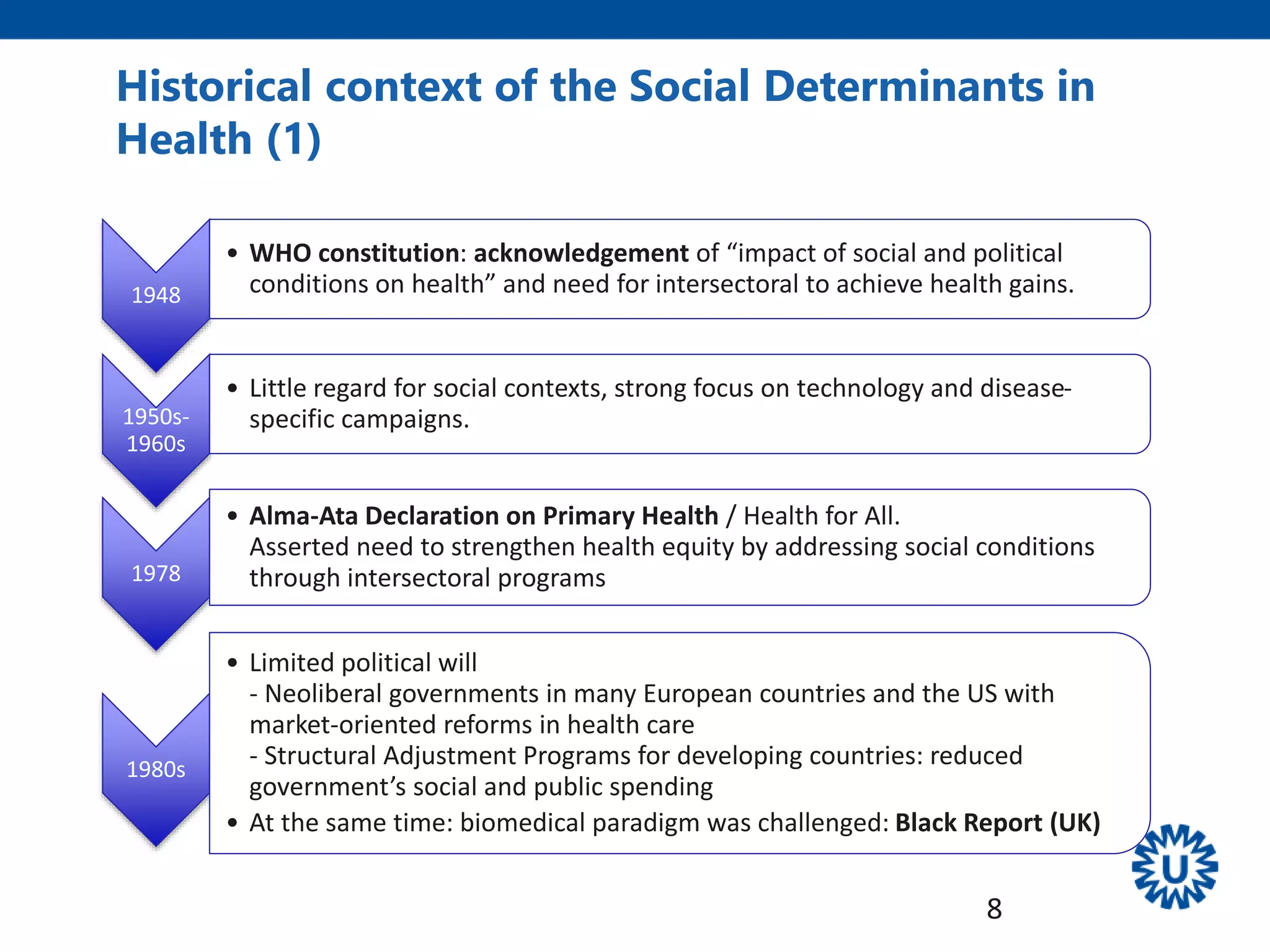
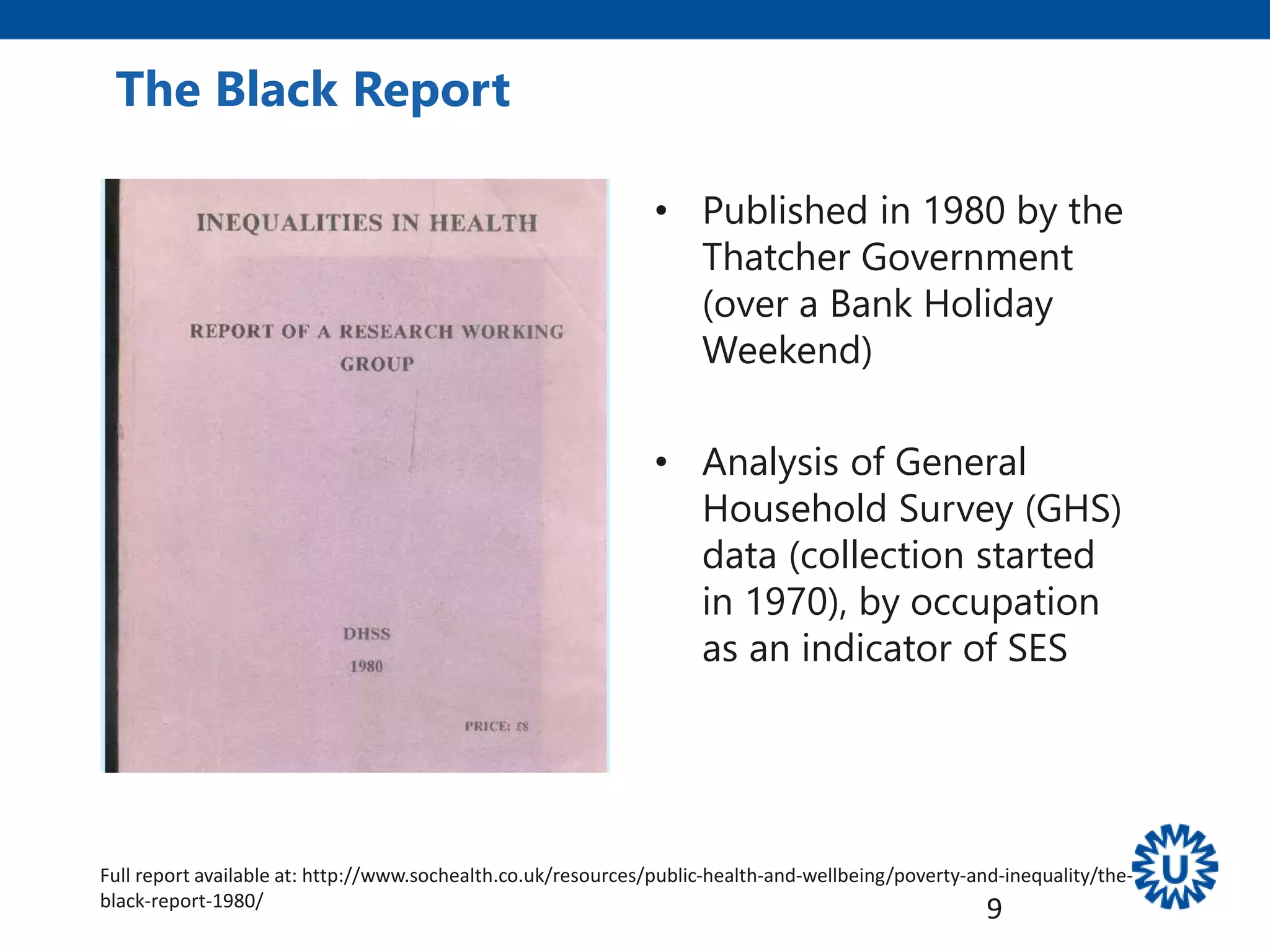
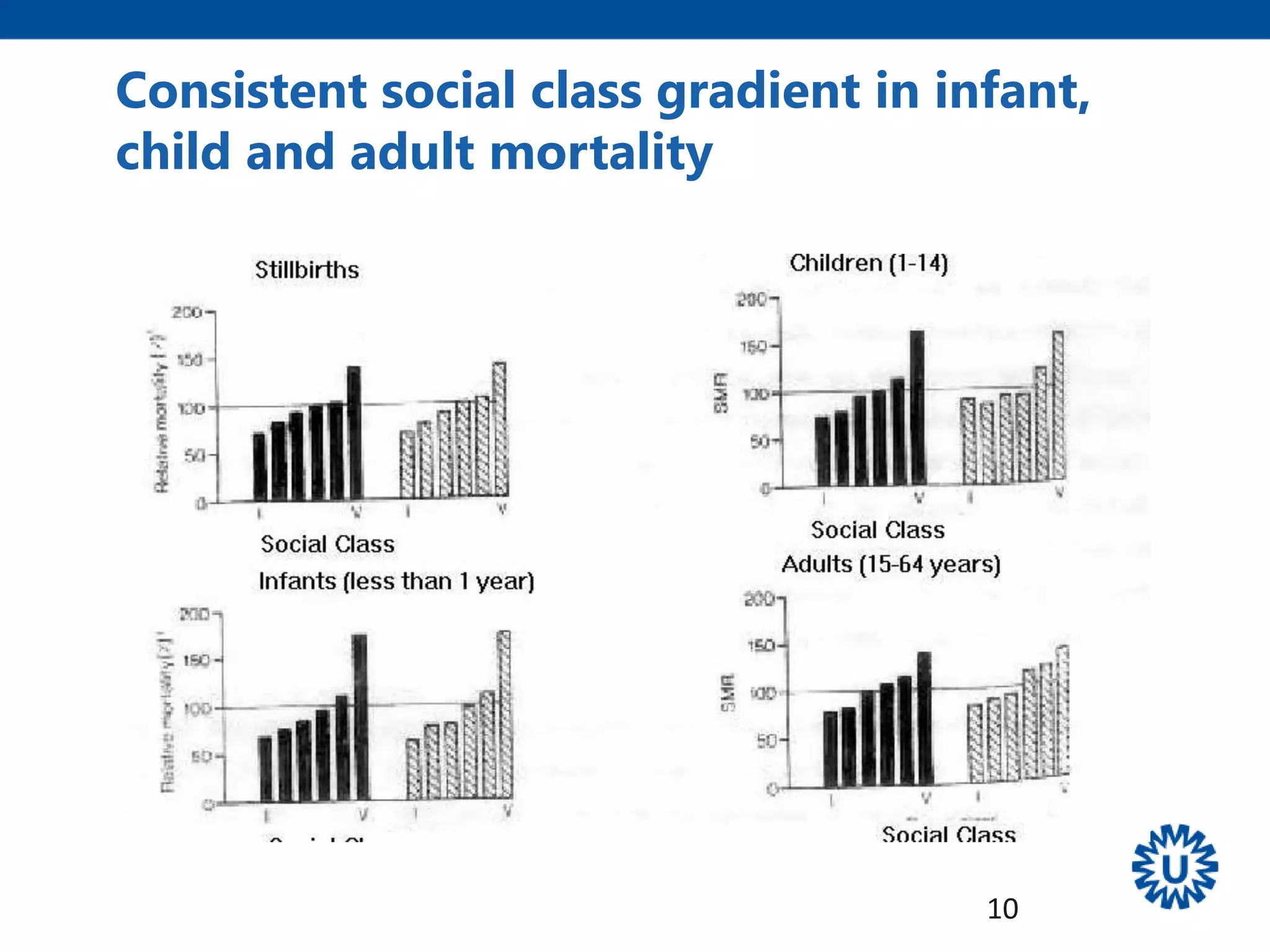
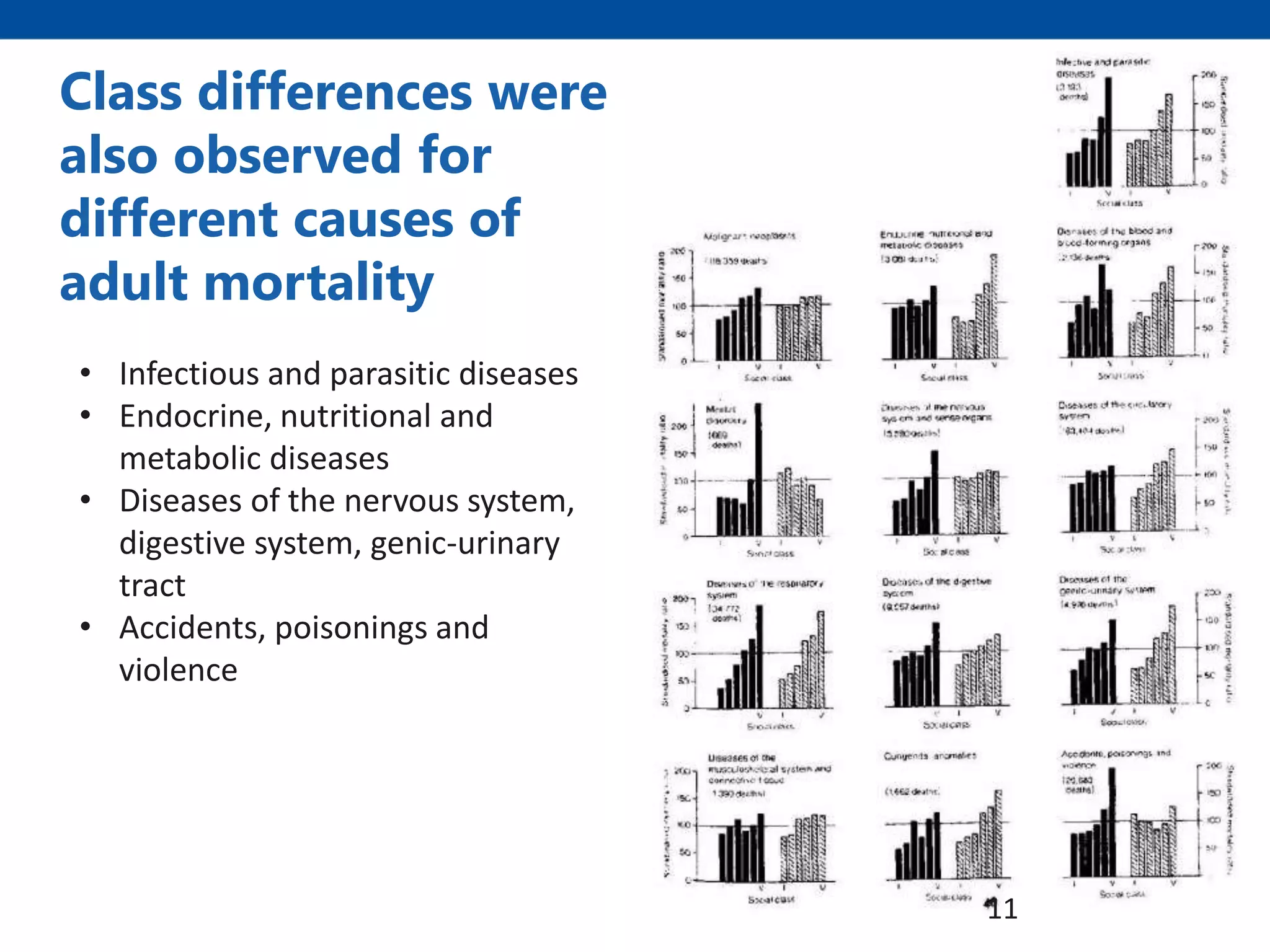
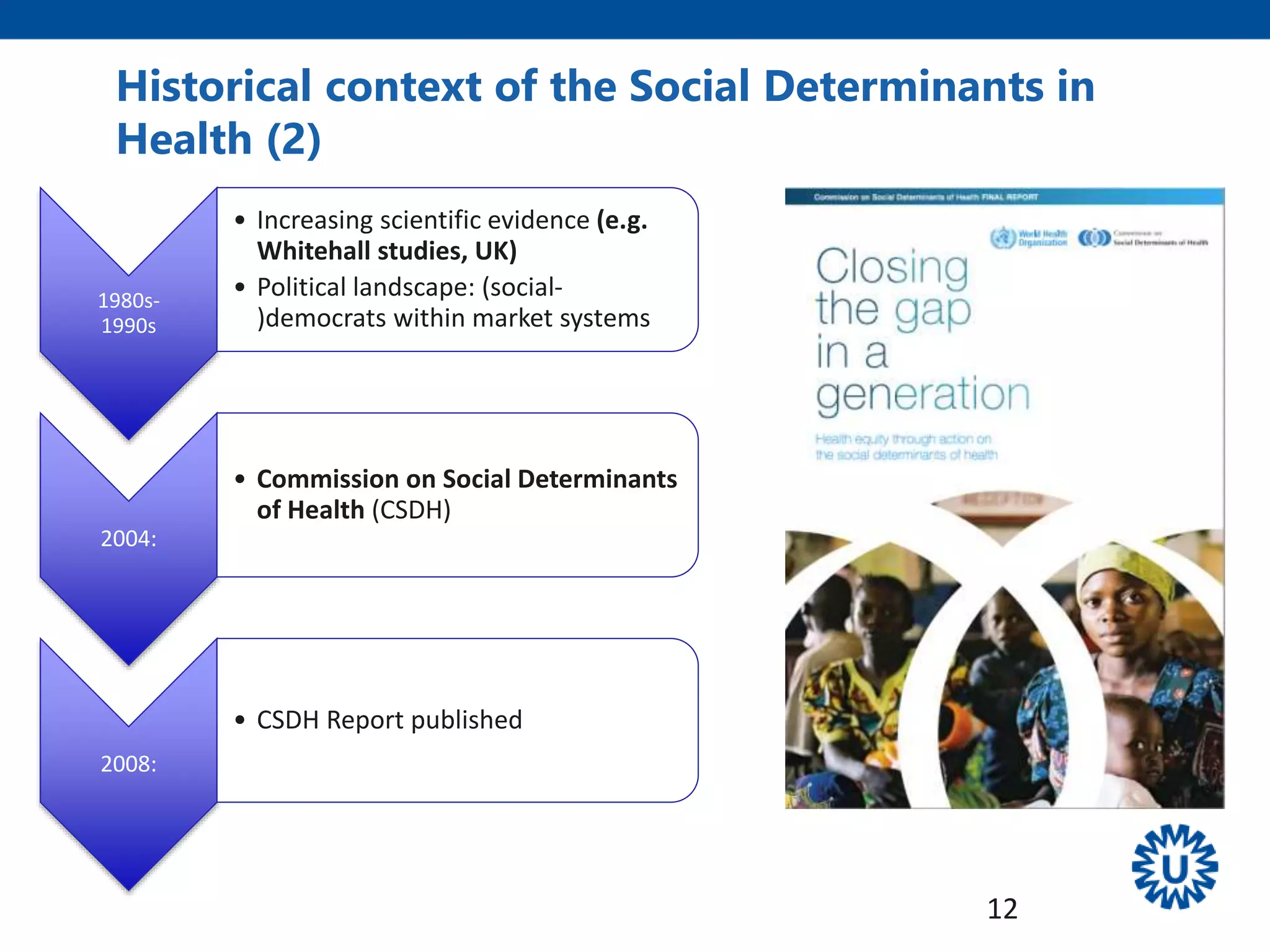
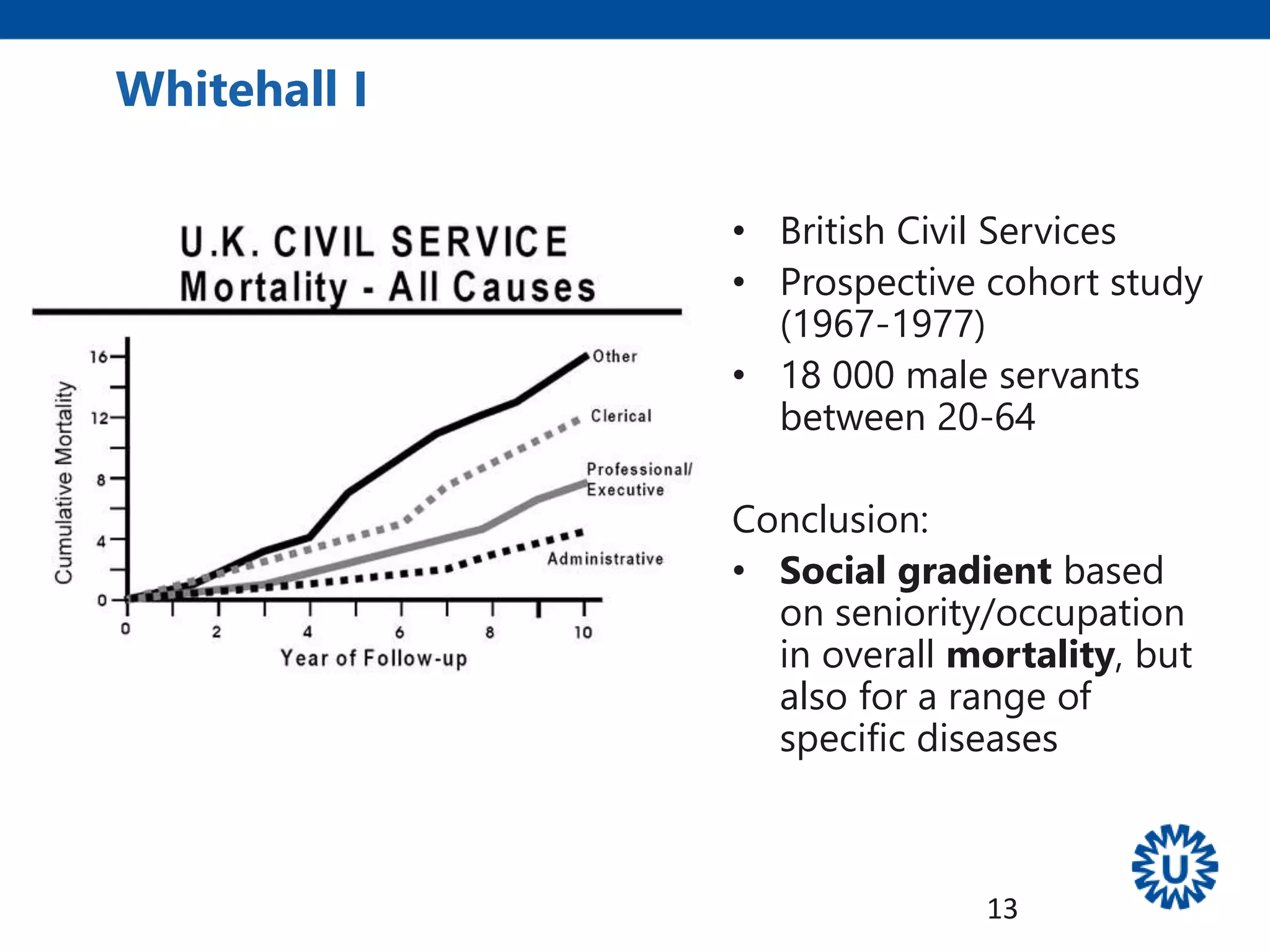
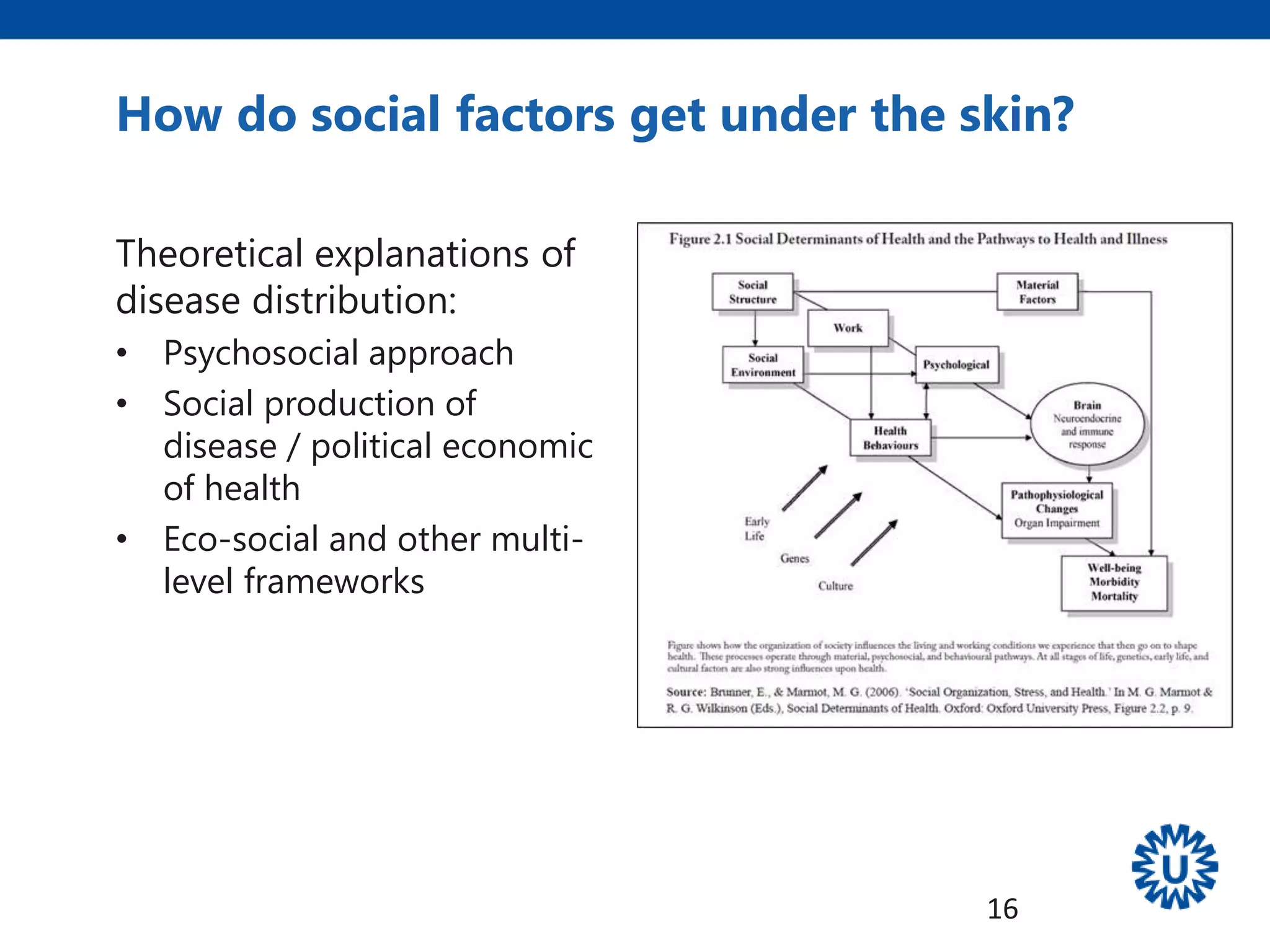
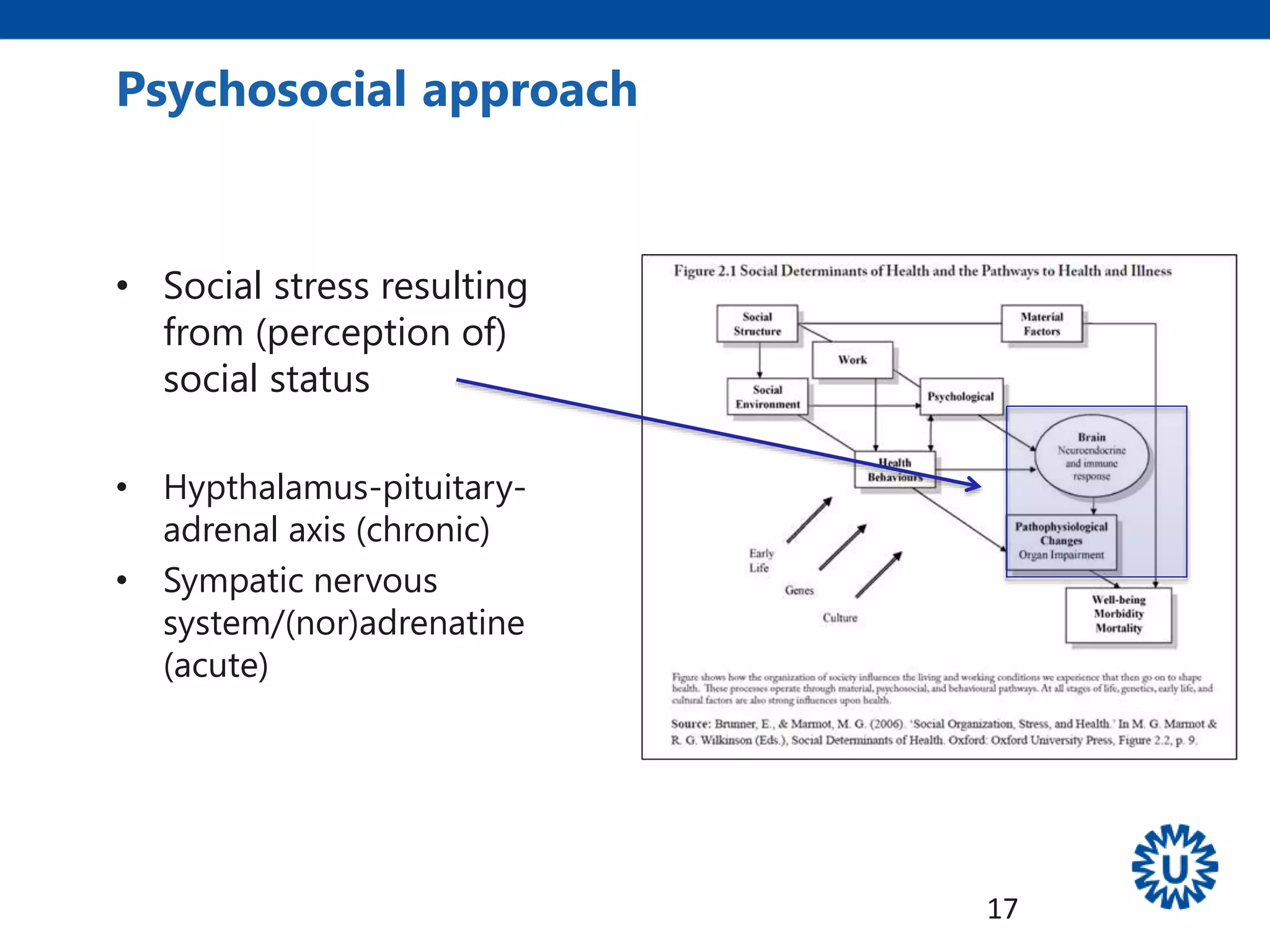
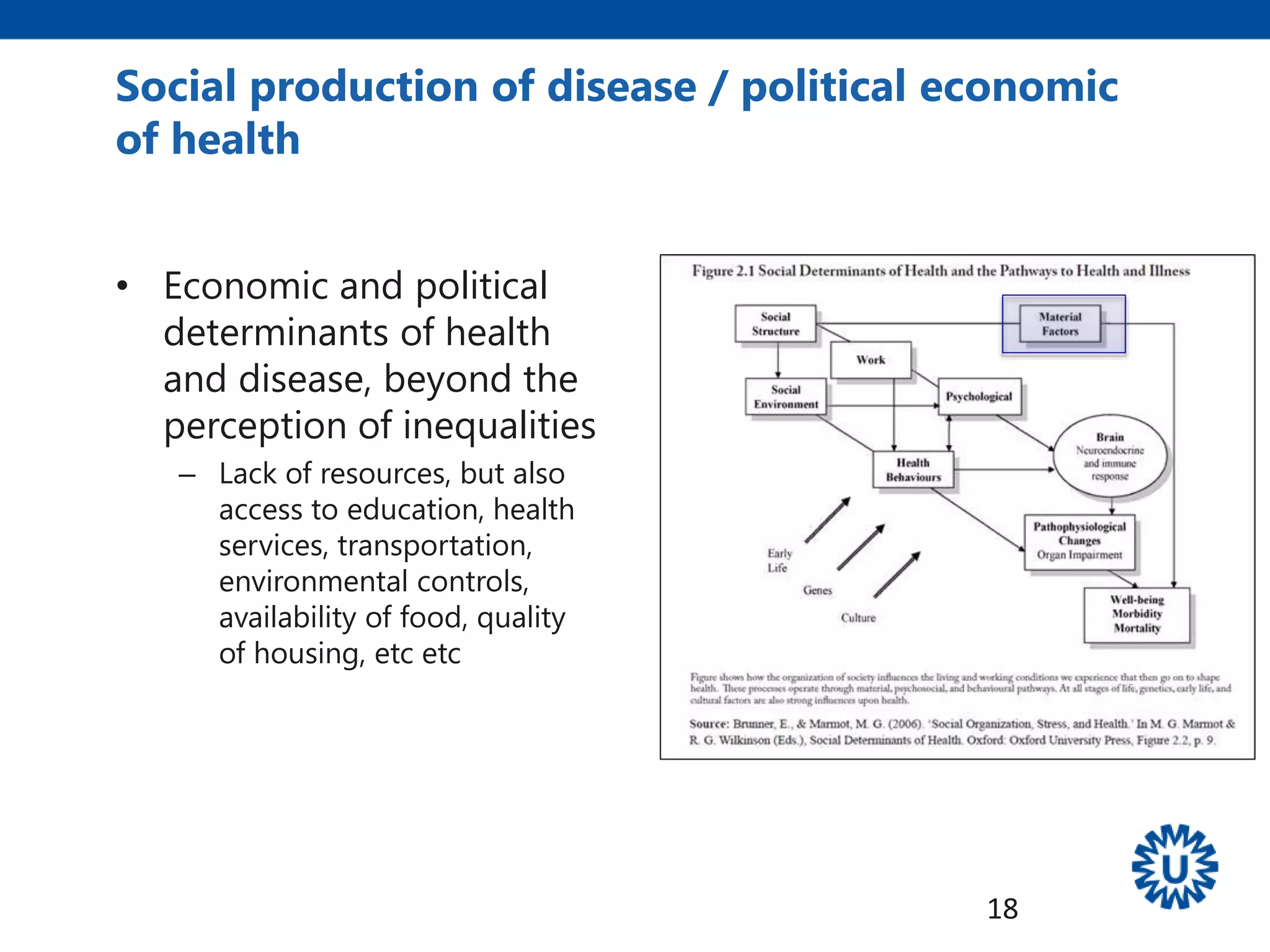
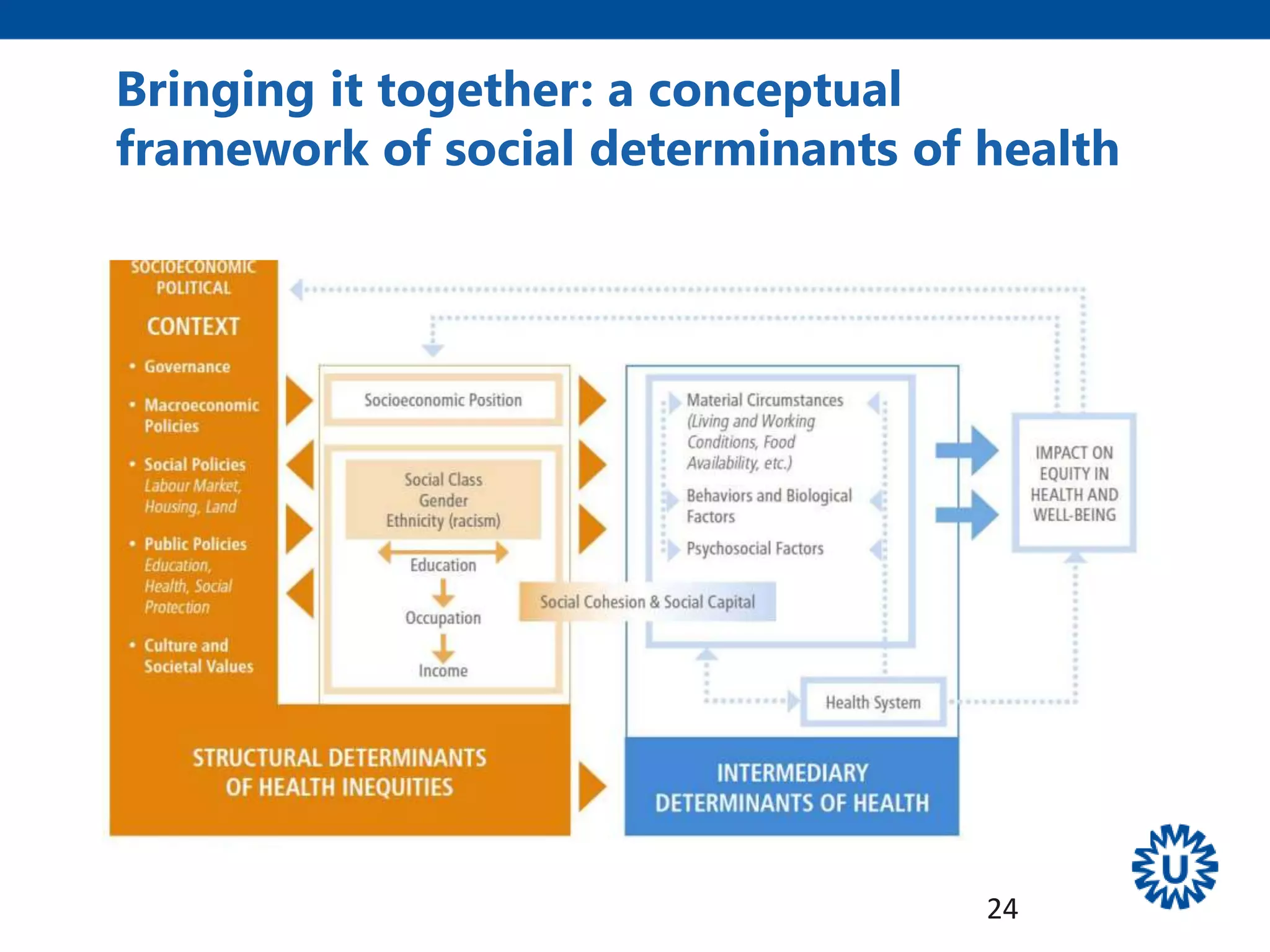
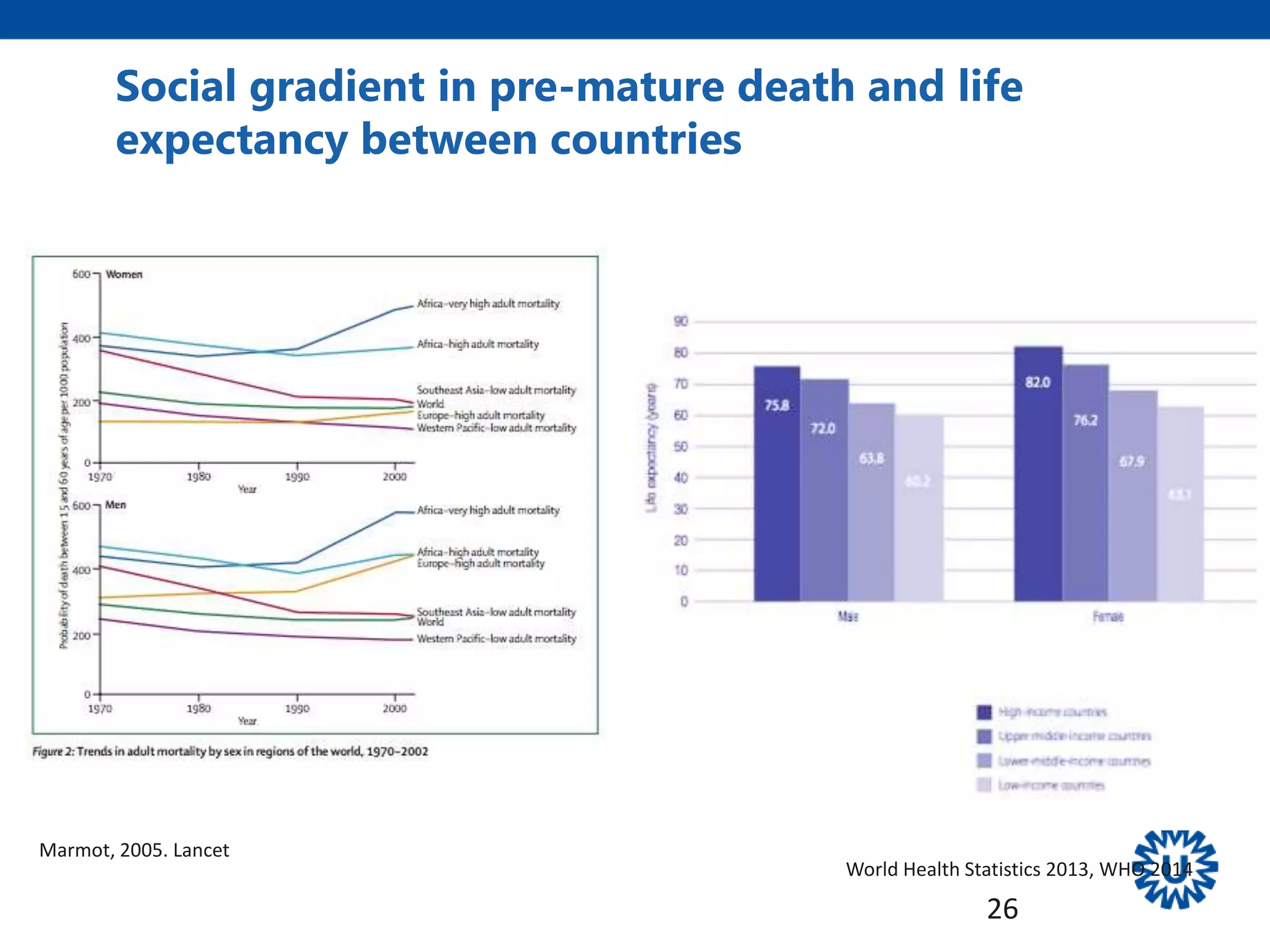
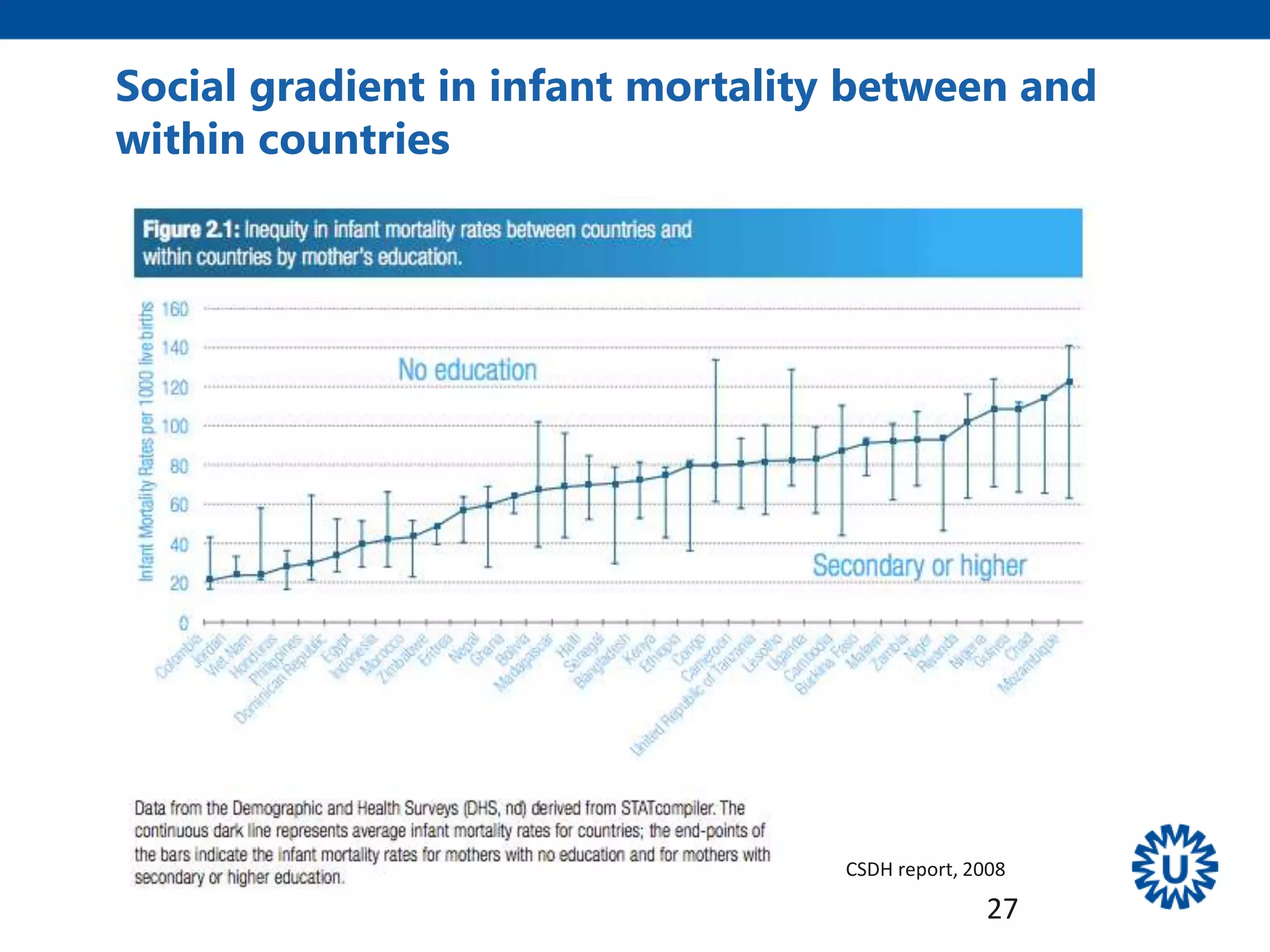
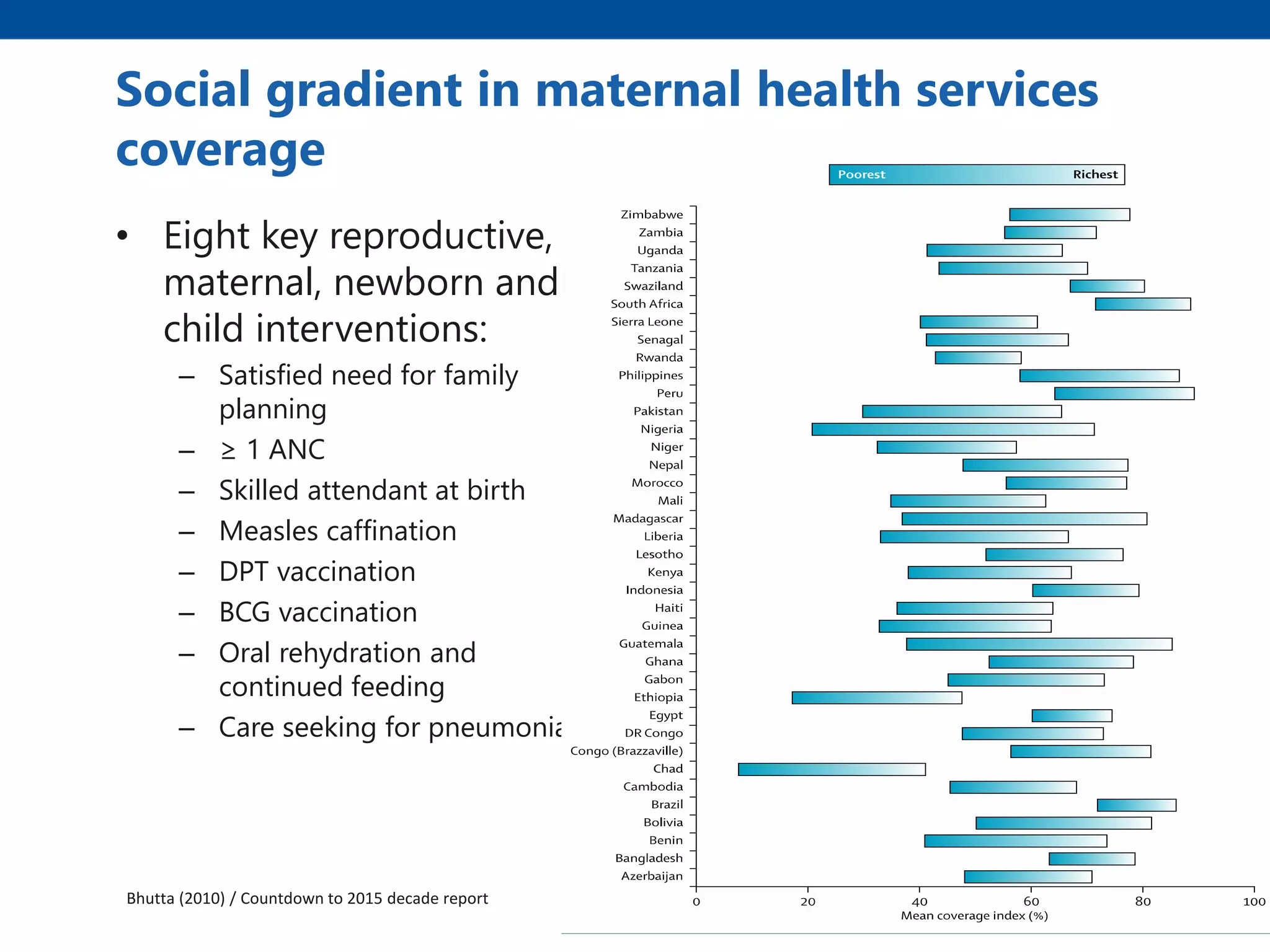
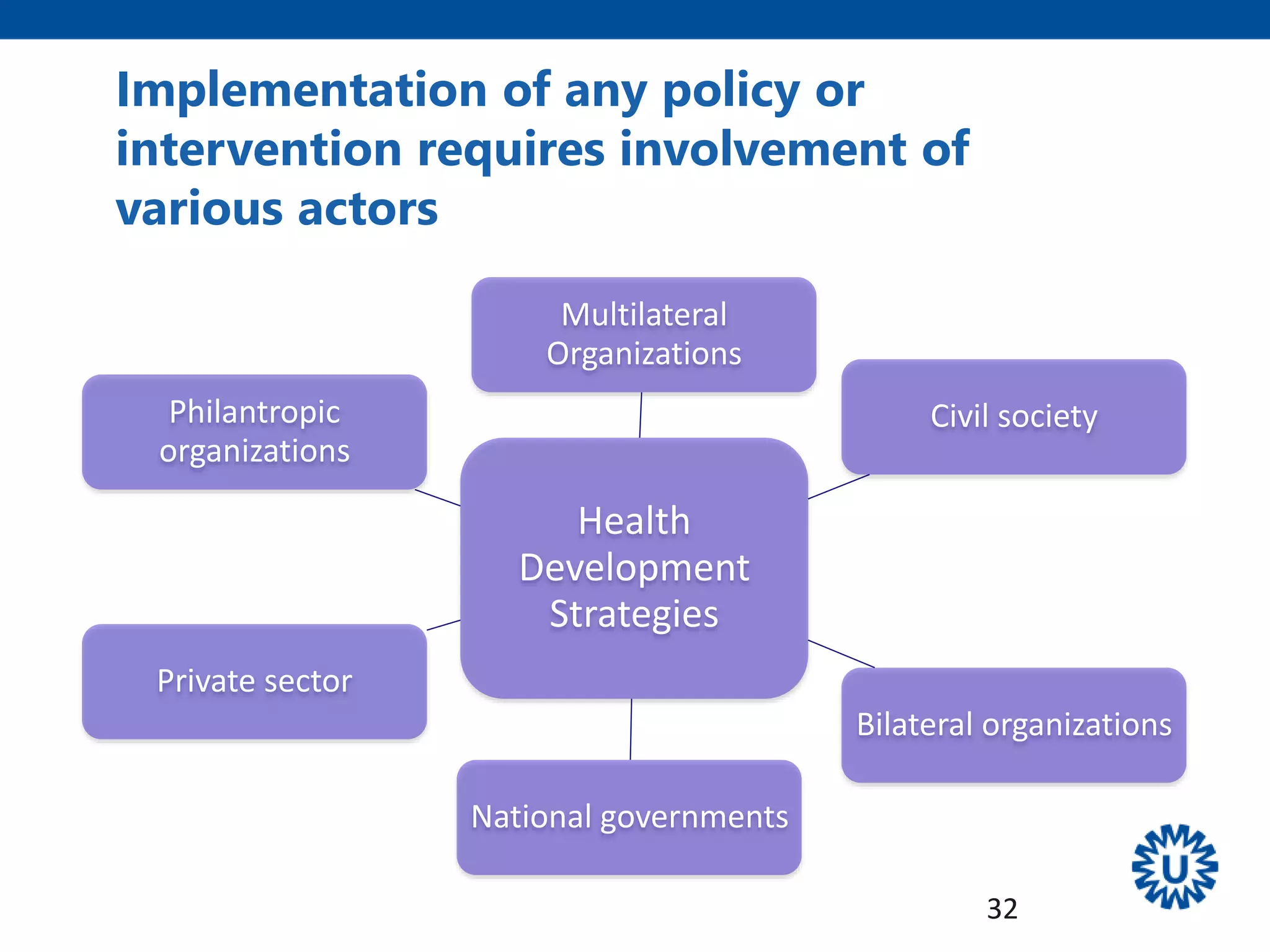
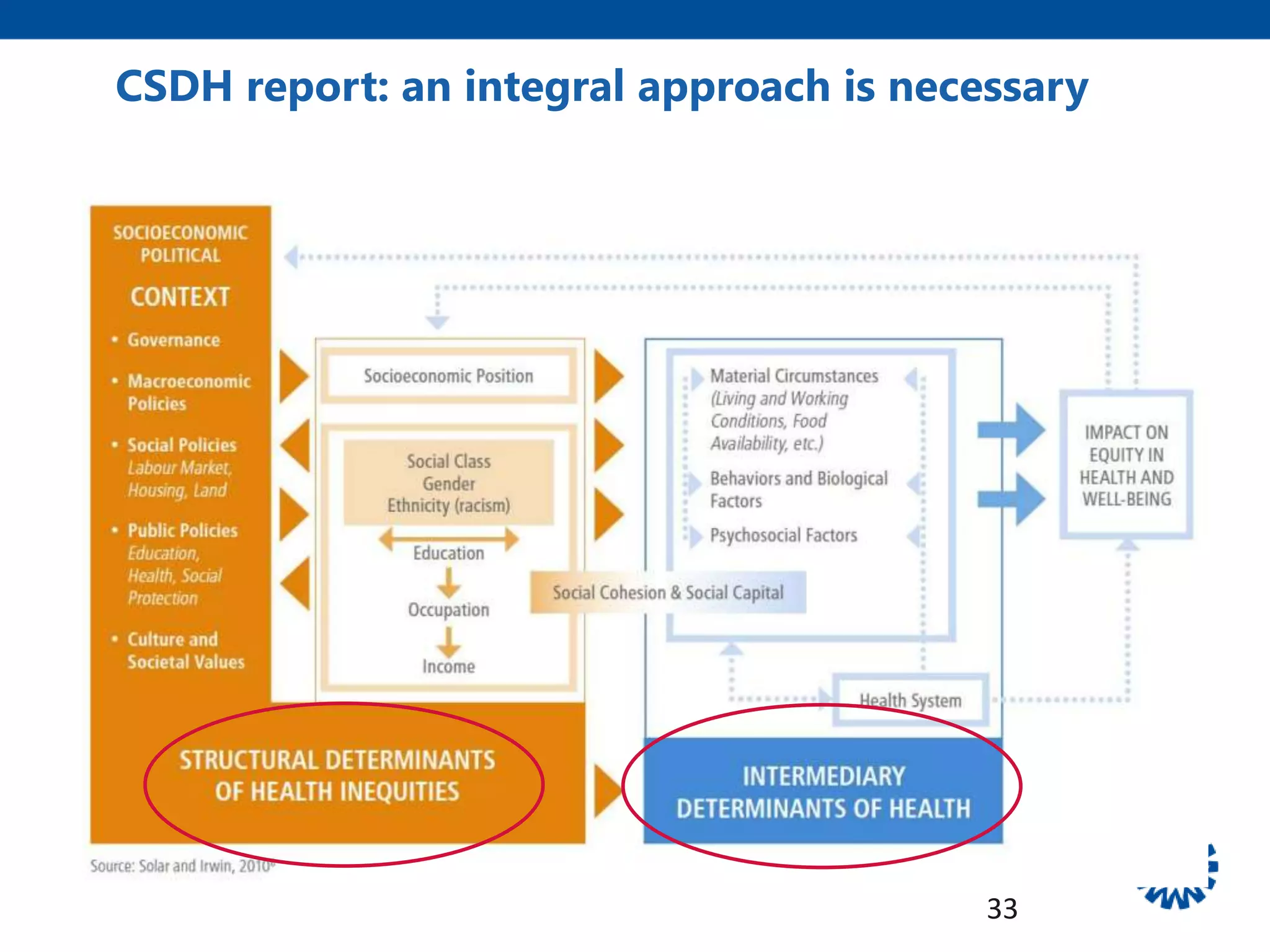
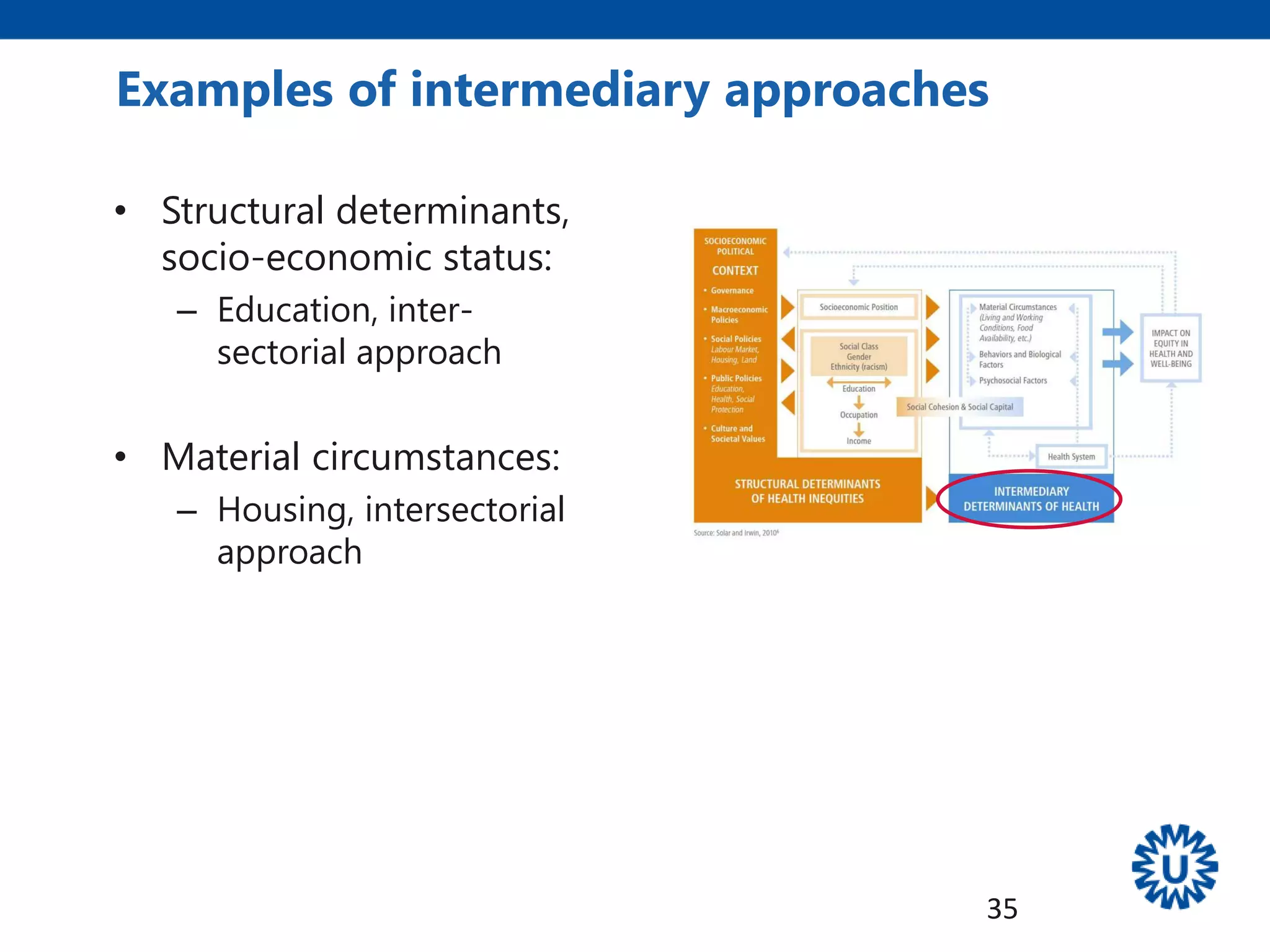
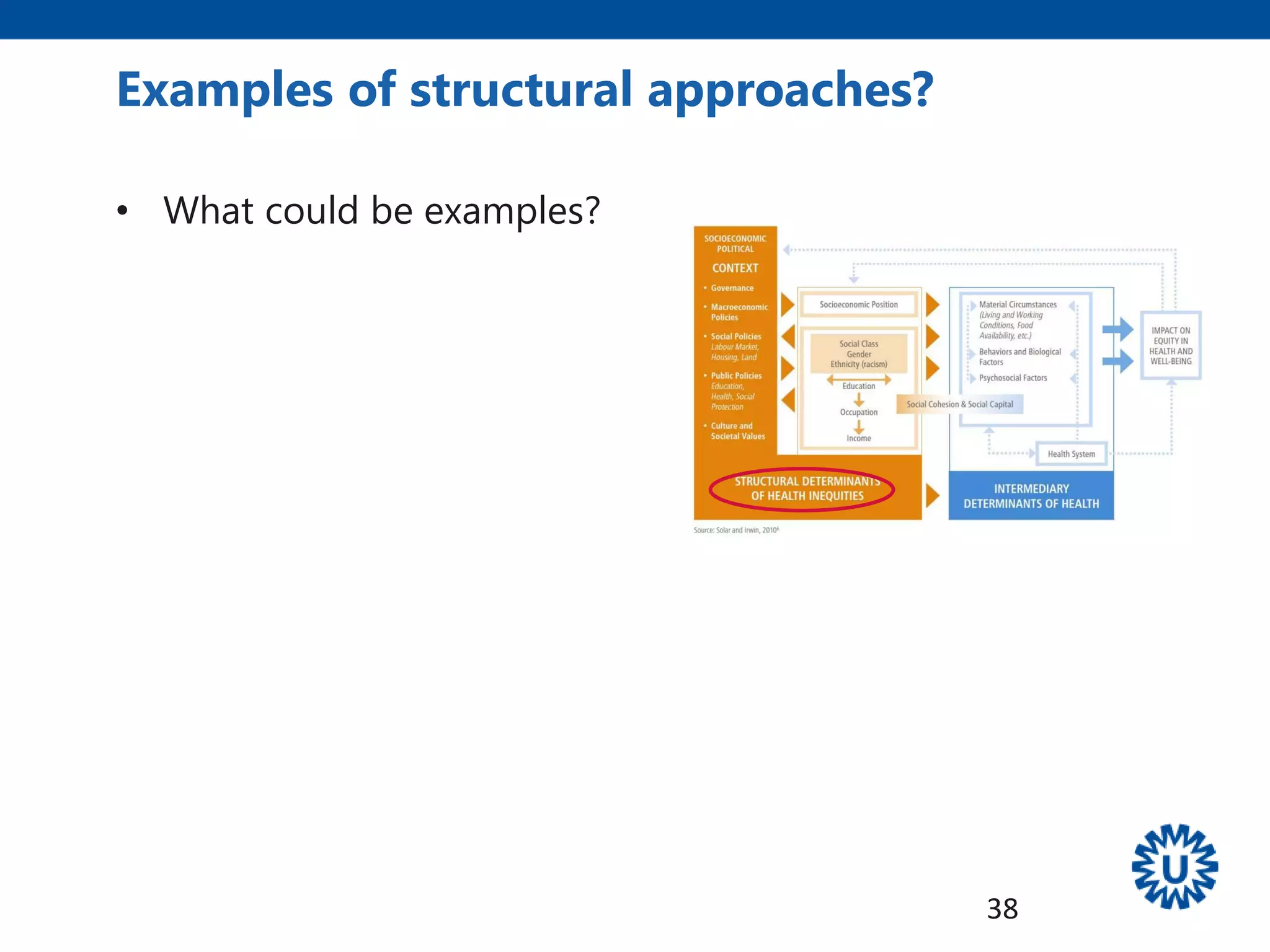
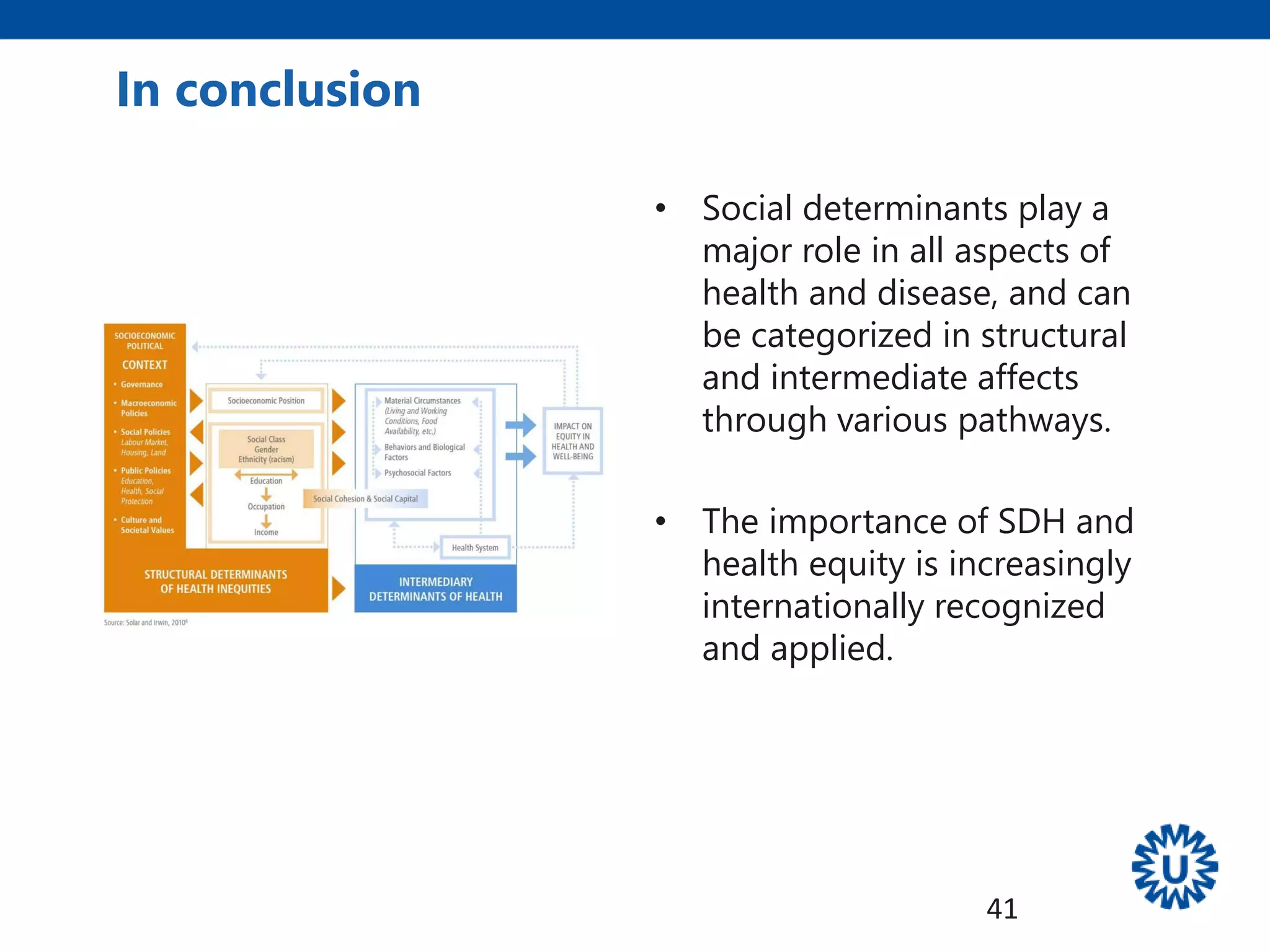
The document discusses social determinants of health, which are defined as the circumstances in which people are born, grow, live, work and age that impact health outcomes. These circumstances are shaped by wider social, economic and political forces. Historical evidence from studies like the Black Report and Whitehall studies showed social gradients in health according to factors like socioeconomic status and occupation. Theoretical frameworks explain how social factors influence health through pathways like psychosocial stress and limited access to resources. A conceptual framework outlines how structural factors like income and education act through intermediate factors like housing and healthcare access to impact health. Addressing social determinants requires multisectoral approaches and involvement of various stakeholders.