1. The document discusses snake bites in Bangladesh, providing information on common poisonous snakes, symptoms of envenomation, and treatment guidelines.
2. It notes that the annual incidence of snake bites in Bangladesh is estimated at 623 per 100,000 people and the mortality from neurotoxic snake bites is significant.
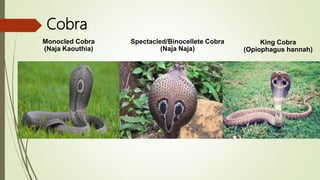
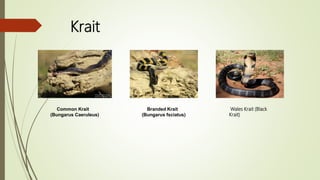
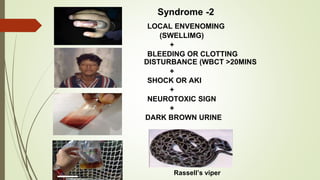
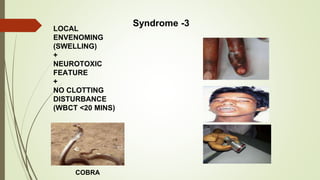
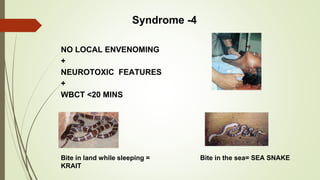
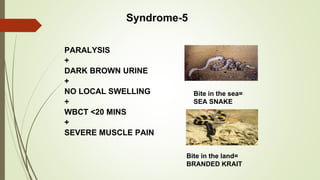
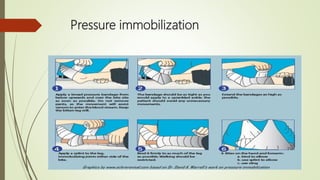
3. Treatment recommendations include reassurance, immobilization of the bitten limb, rapid transfer to the hospital, 20 minute whole blood clotting test to identify venom-induced coagulopathy, and administration of antivenom for systemic envenomation symptoms from cobra, krait, Russell's viper, and saw-scaled viper bites.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









