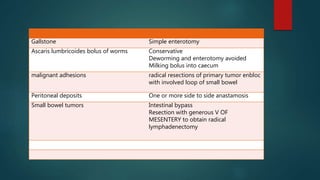
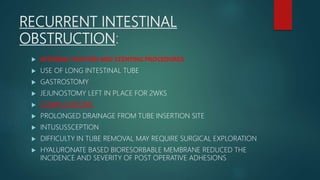
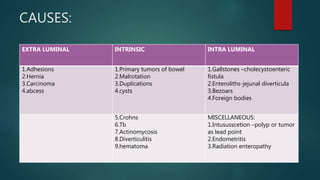
This document discusses the causes, pathophysiology, symptoms, diagnosis, complications and treatment of small bowel obstruction. The causes are categorized as extra-luminal, intra-luminal, and intra-abdominal. Adhesions are the most common cause. The pathophysiology involves dehydration, electrolyte imbalances, and potential ischemia. Symptoms include colicky abdominal pain, nausea, vomiting, distension and obstipation. Diagnosis involves imaging like plain radiographs and CT scan. Treatment involves fluid resuscitation, antibiotics, nasogastric decompression, and surgery to remove the obstruction if not resolving. Surgery involves finding and releasing the point of obstruction while assessing bowel viability. Recurrent obstruction can be








![Serum sodium
Chloride
Potssium & creatinine levels checked for
ADEQUACY OF RESUSCITATION
HEMOCRIT VALUE FOR HEMOCONCENTRATION
SUPERCONDUCTING QUANTUM INTER FERENCE
DEVICE [SQUID ] MAGNETOMETER –MESENTERIC
ISCHEMIA
BER CHANGES – INTESTINA ISCHEMIA
ELEVATION OR ABSENCE OF LEUCOCYTOSIS
DOES NOT R/O STRANGULATION
LABORATORY TESTS](https://image.slidesharecdn.com/siobstruction-200819113419/85/Small-bowel-obstruction-obstruction-10-320.jpg)