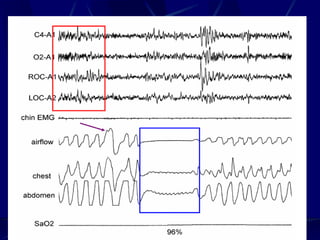
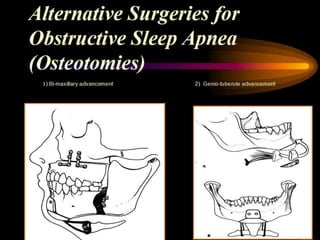
Obstructive sleep apnea (OSA) involves cessation of breathing during sleep due to collapse of the upper airway. The document discusses the history, types, prevalence, risk factors, symptoms, diagnosis and treatment of OSA. Regarding treatment, positive airway pressure with CPAP is very effective but requires good mask fit and humidification. Surgery and oral appliances can also be used but may not be curative. Lifestyle changes like weight loss and avoiding alcohol before bed can help reduce OSA severity. Untreated OSA is associated with increased risk of health issues like hypertension.






![OBSTRUCTIVE SLEEP APNEA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstructivesleepapneaautosaved-240801041633-6b724373-thumbnail.jpg?width=640&height=640&fit=bounds)





























































