Downloaded 68 times
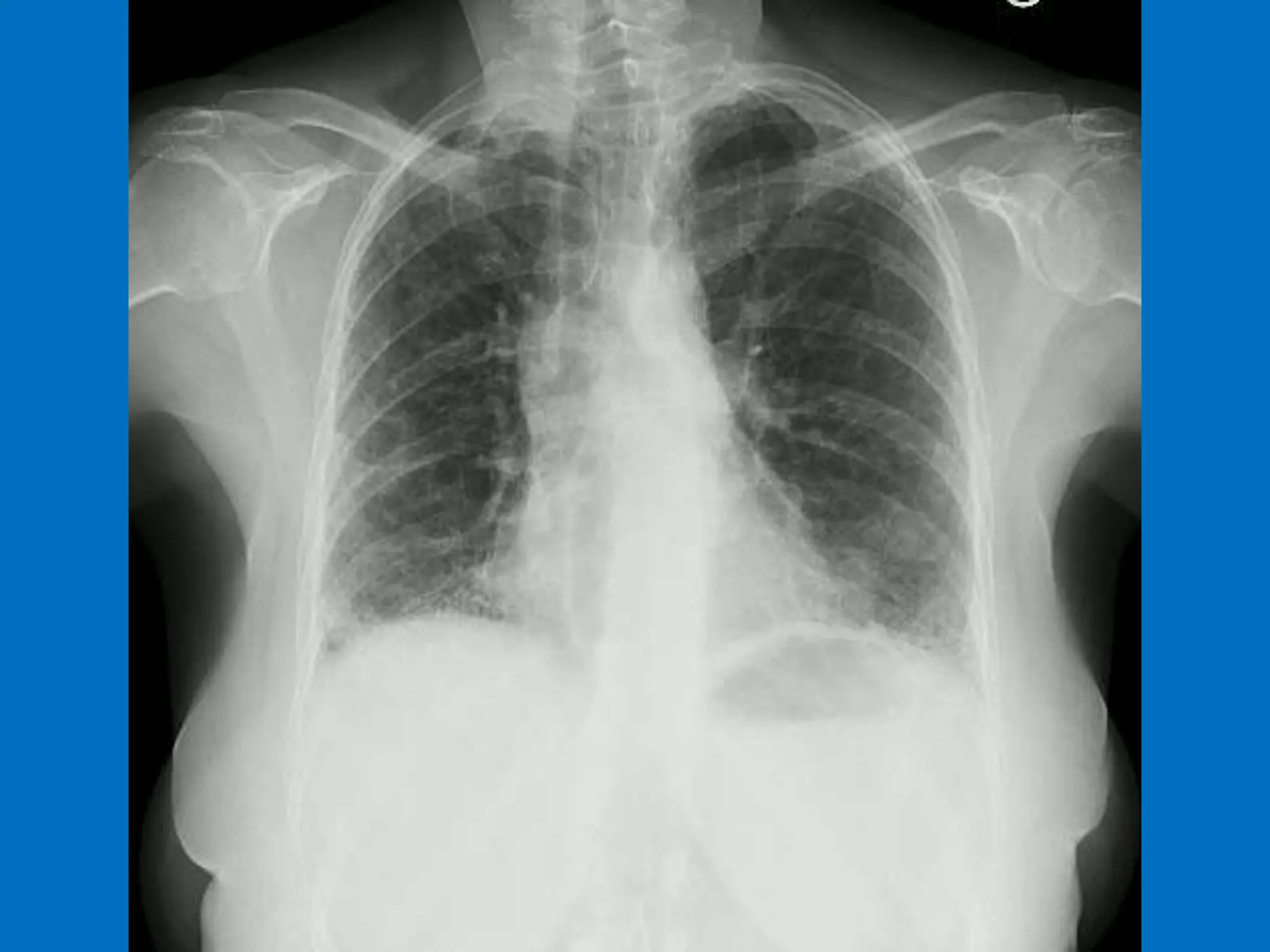

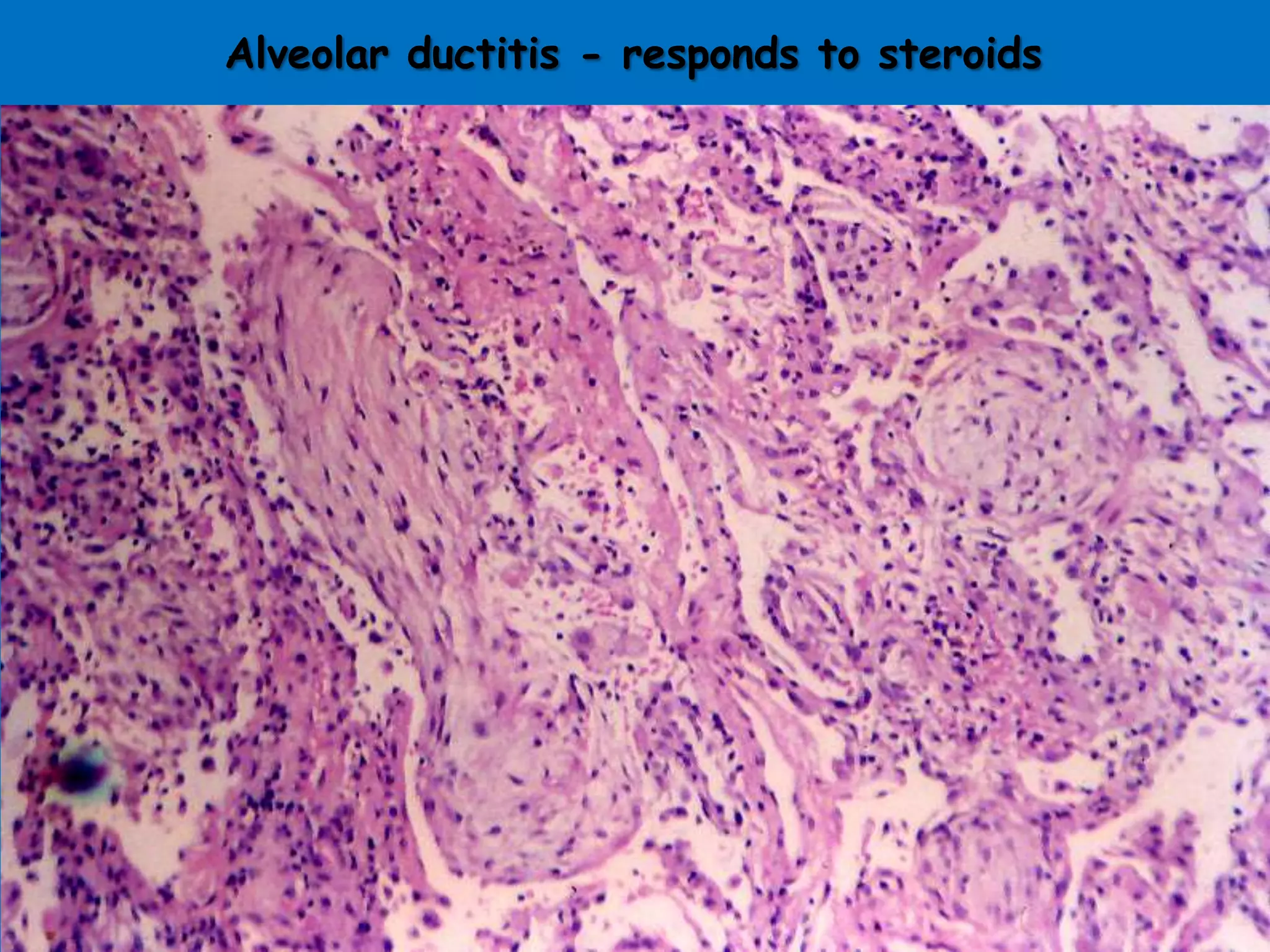
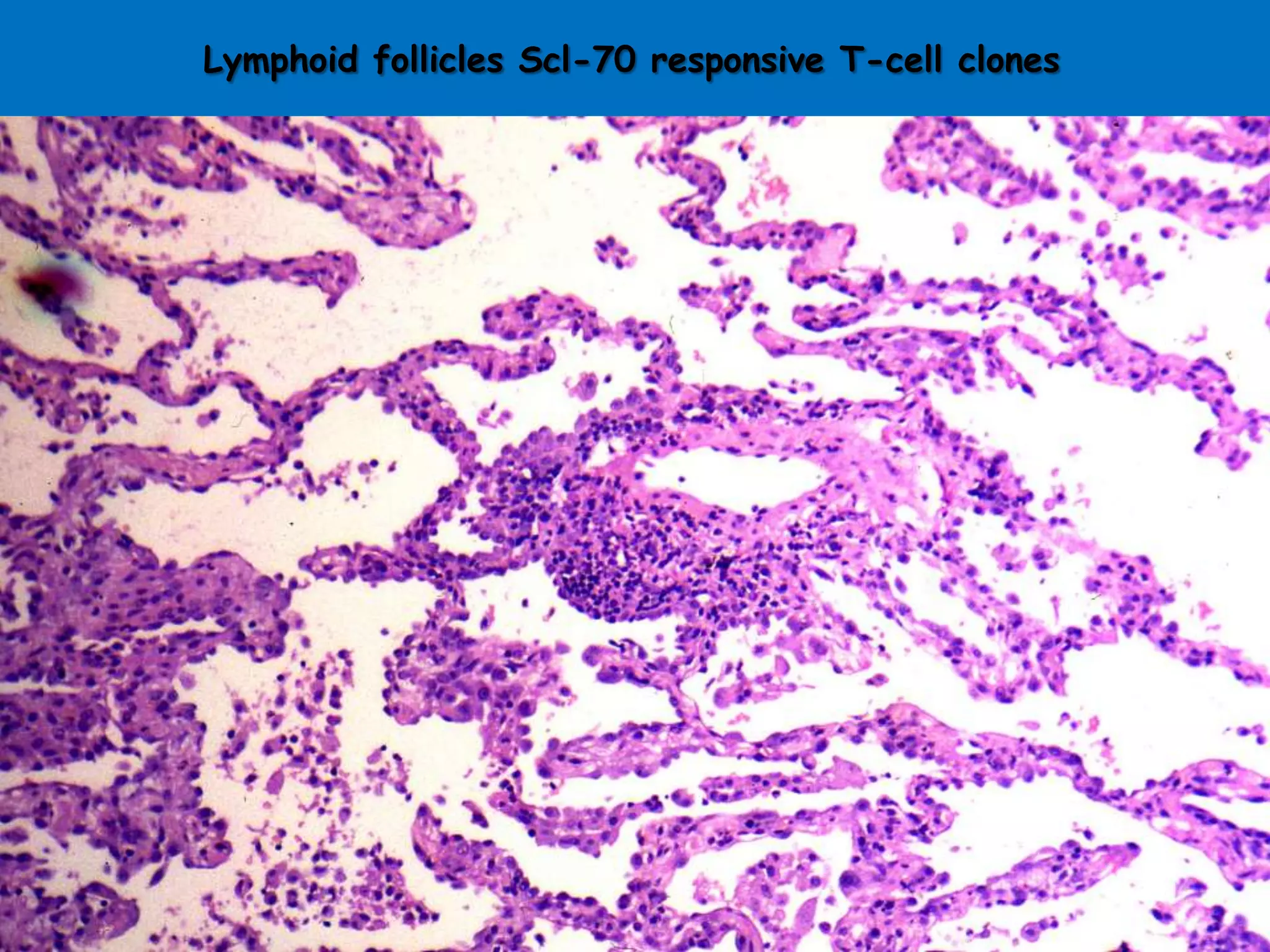
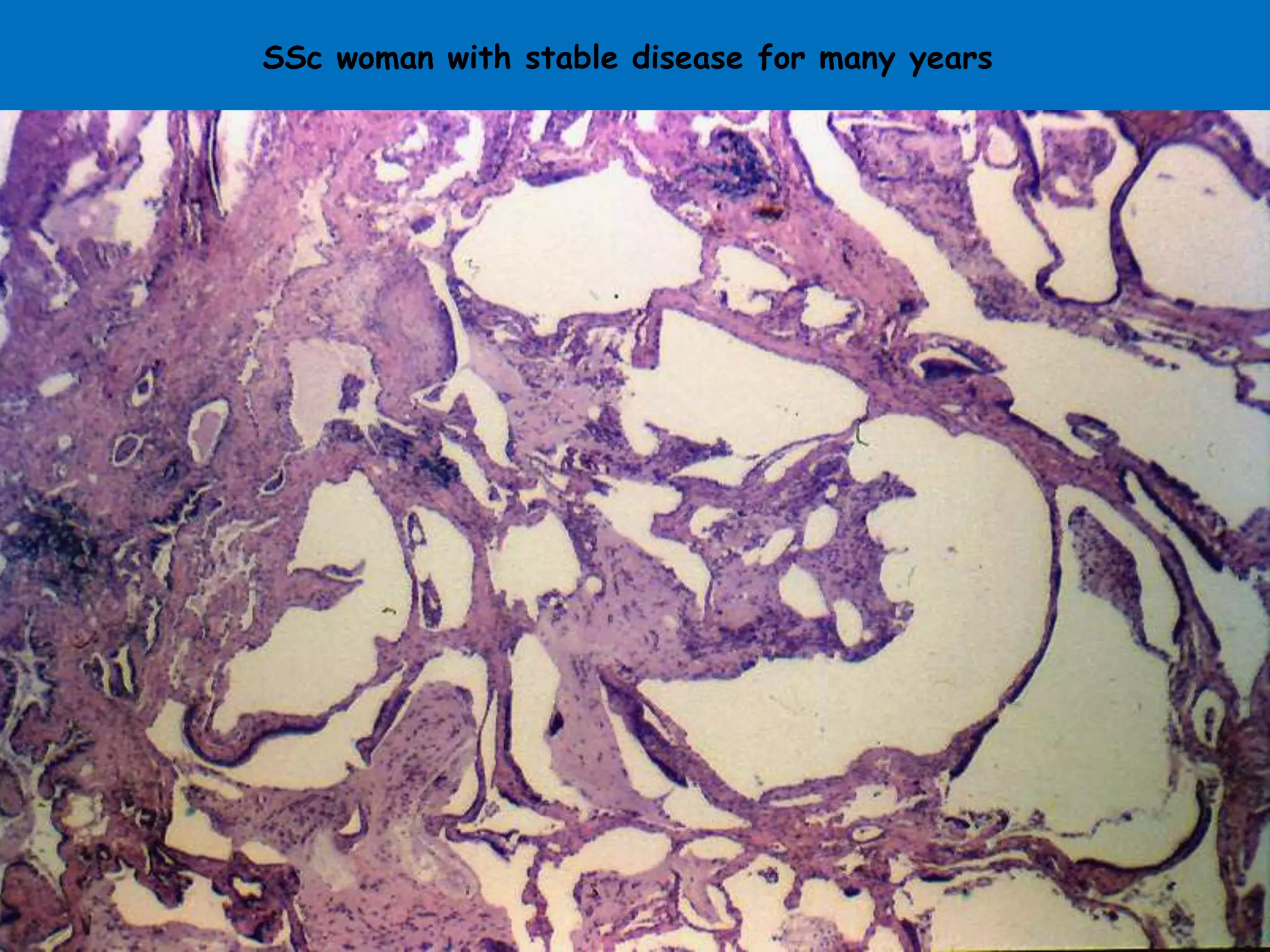





Scleroderma lung disease encompasses various respiratory complications, including interstitial fibrosis and alveolar ductitis, which are prevalent in patients. Recent research has identified differential gene expression in lung fibroblasts and new treatment options like antifibrotic and anti-inflammatory drugs. Despite the challenging prognosis, ongoing studies are promising in elucidating the disease mechanisms and potential therapeutic targets.