Download to read offline


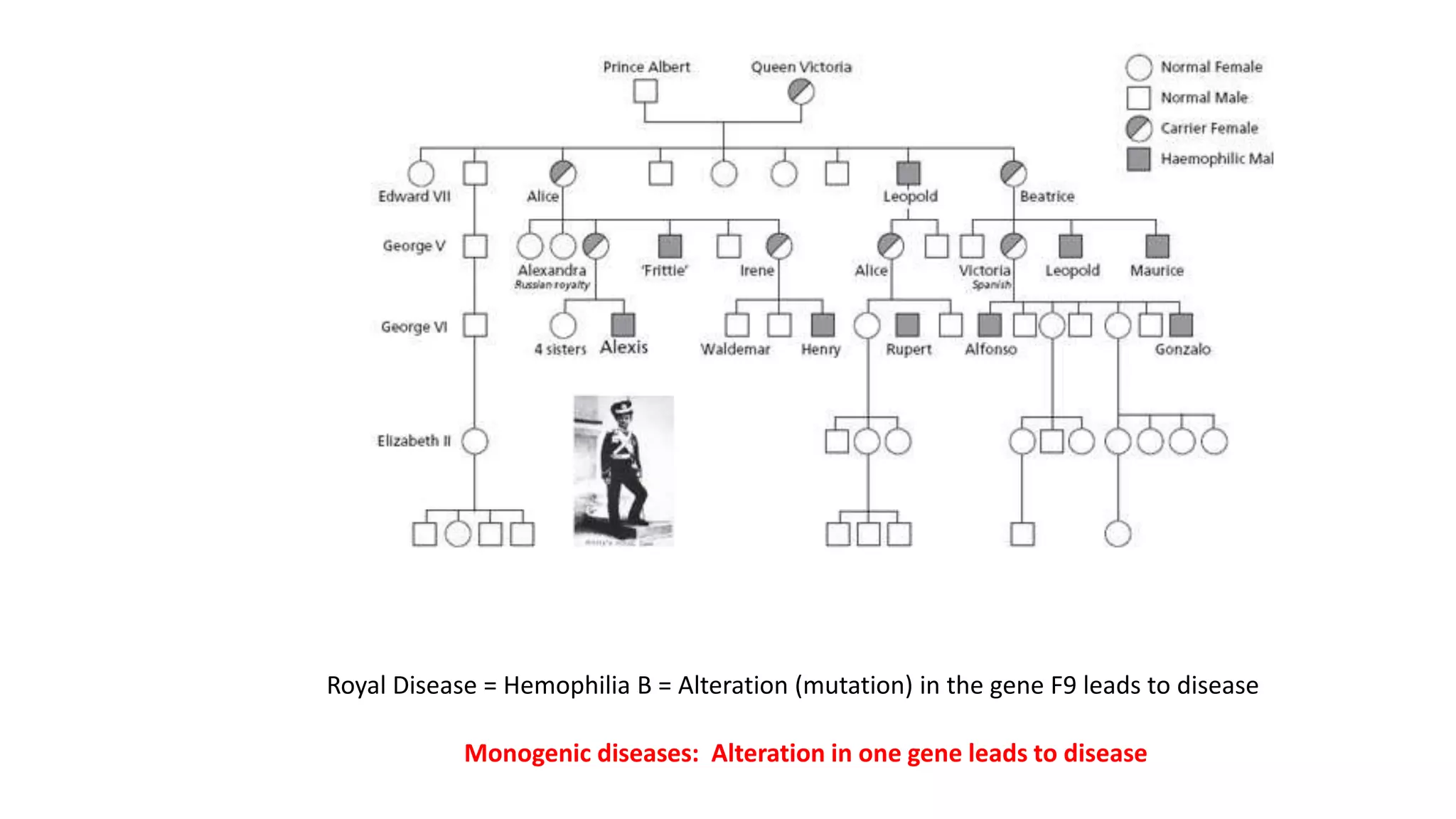
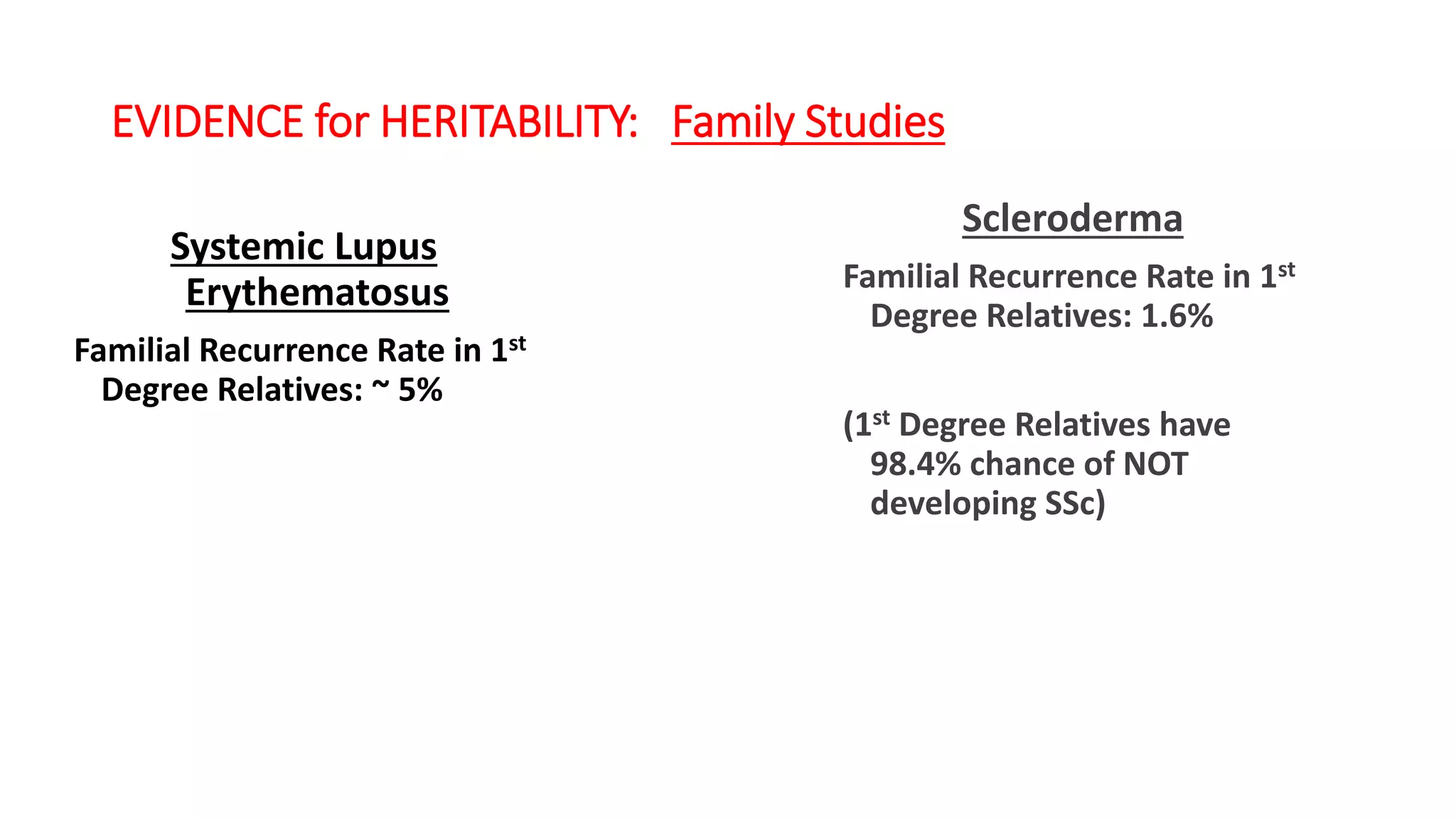
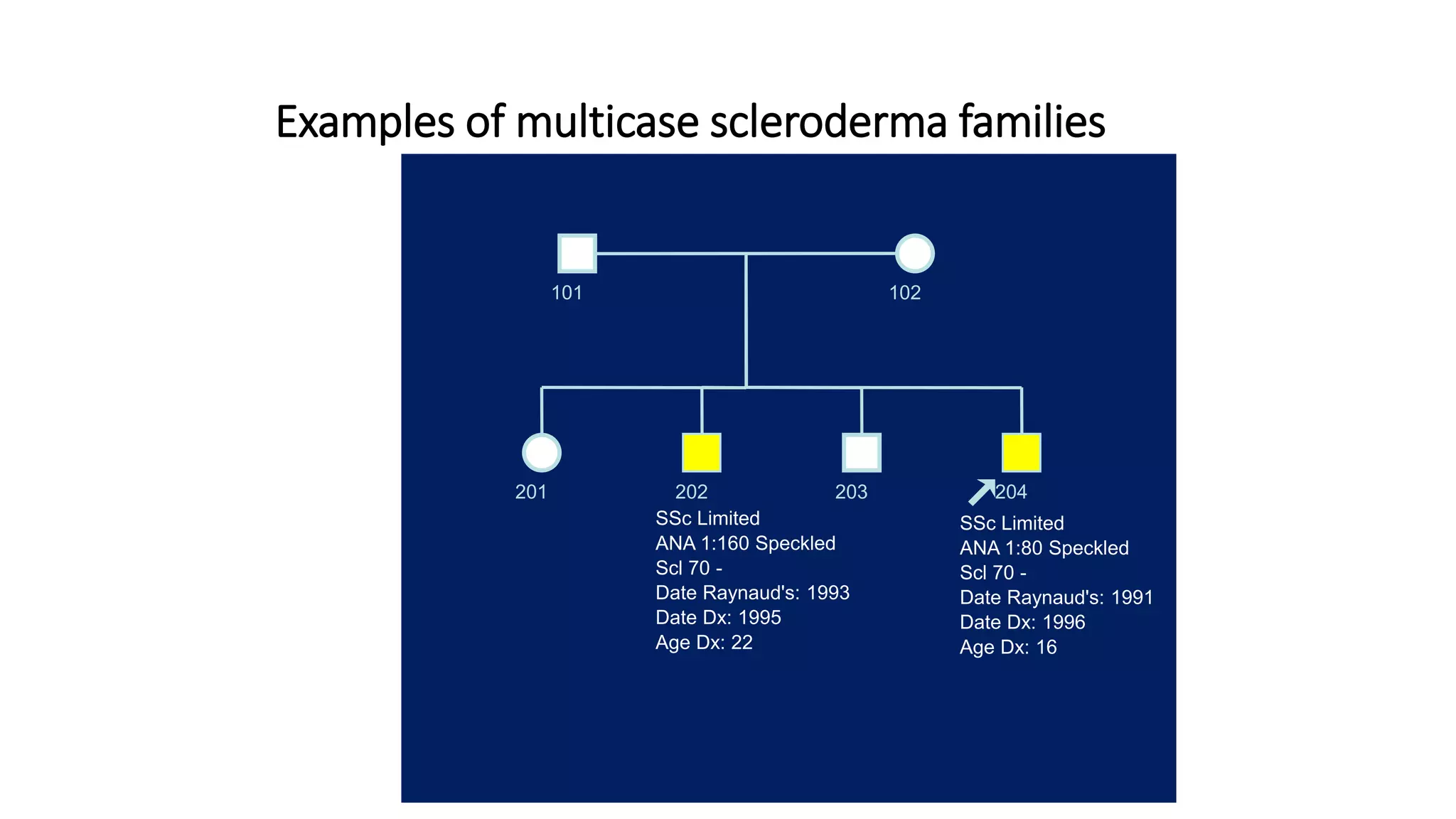
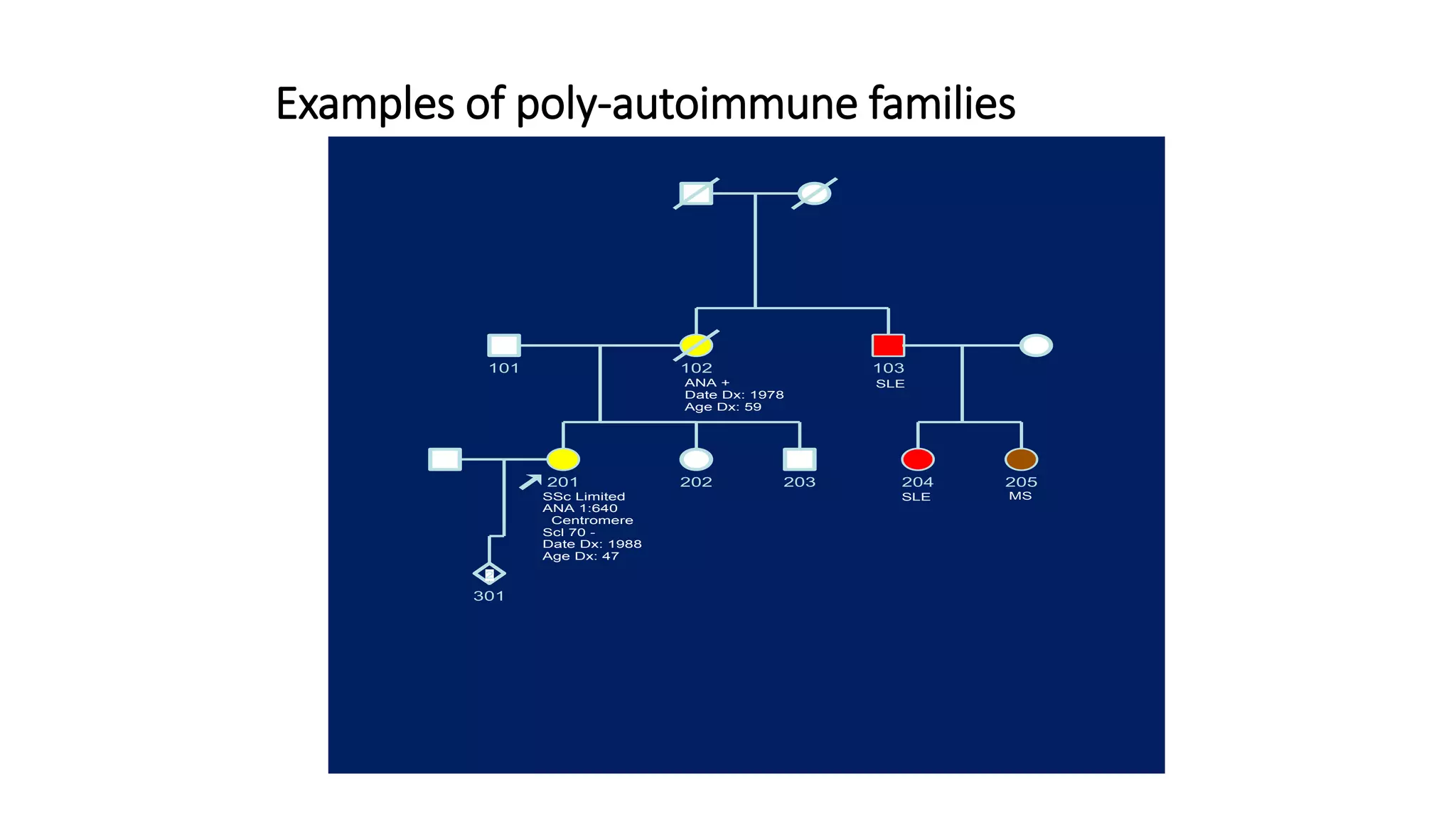
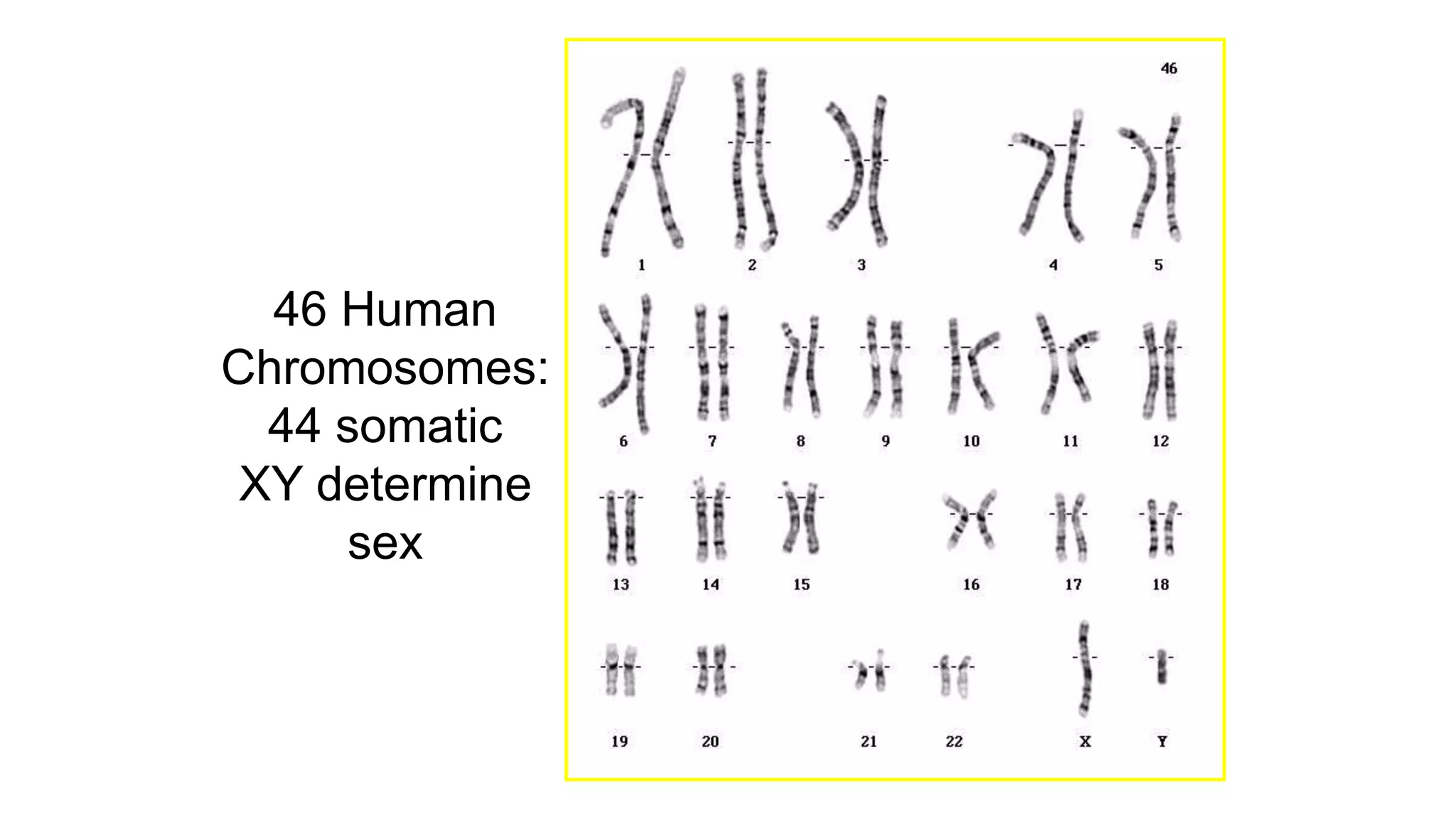
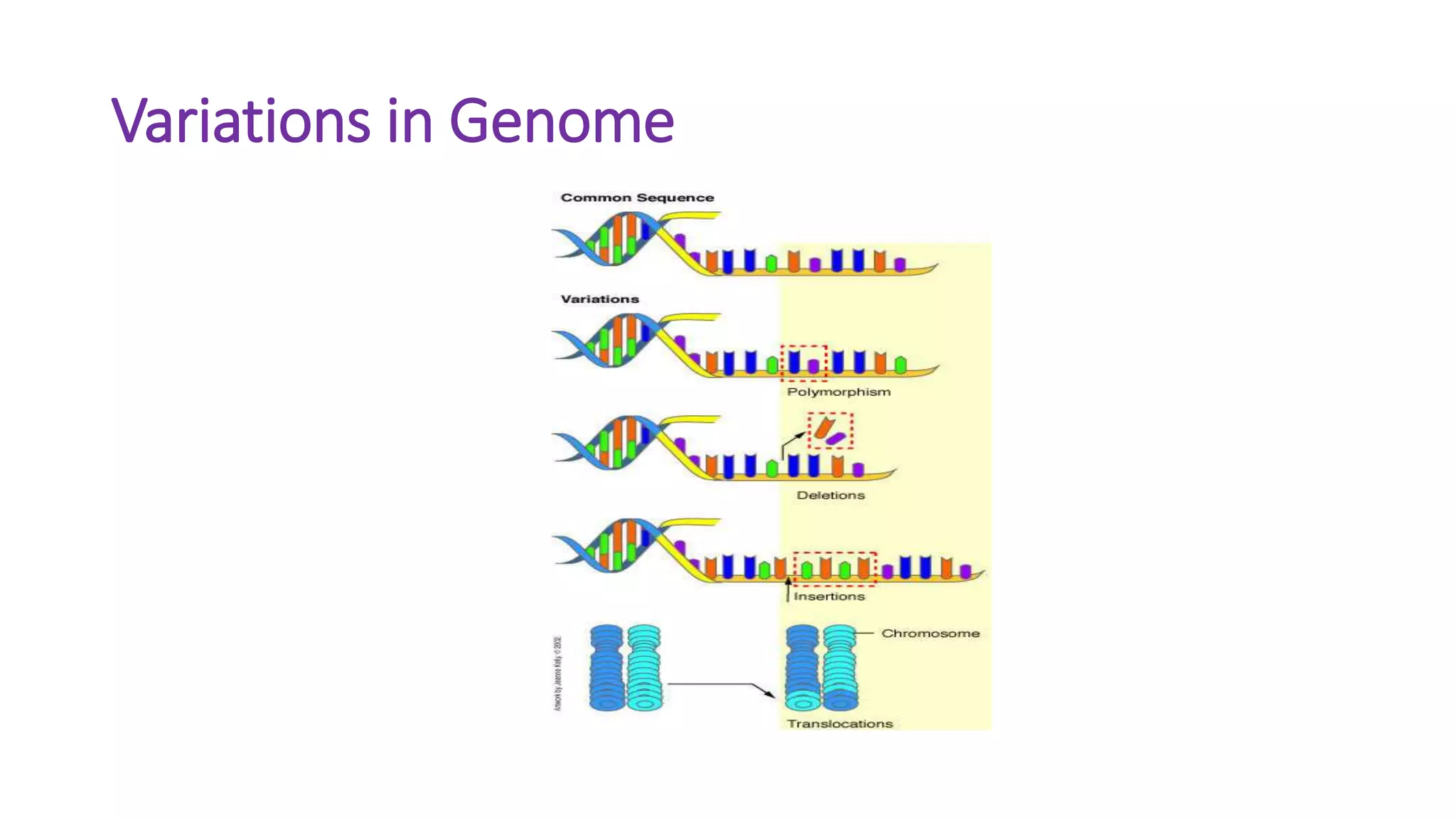
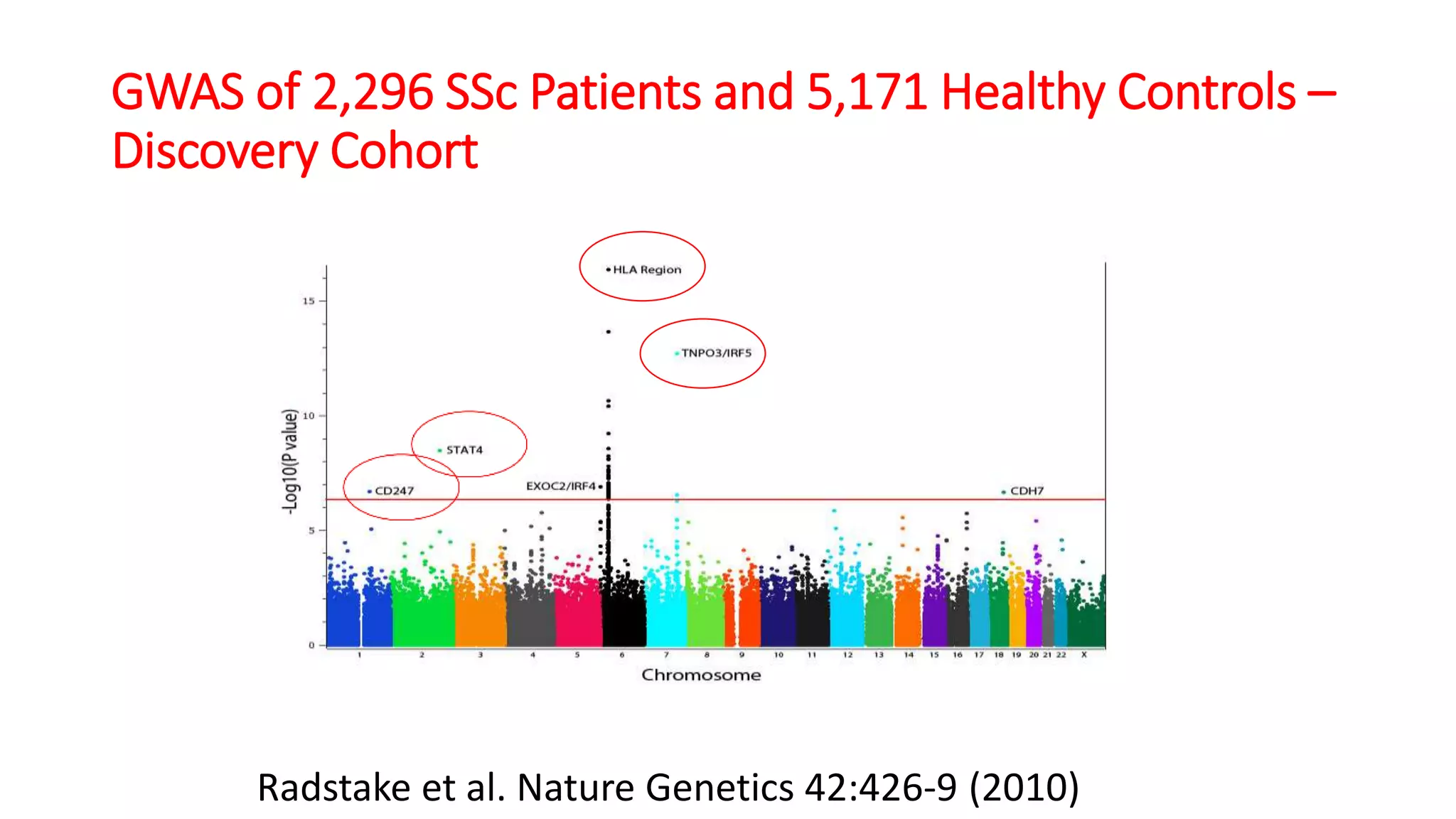
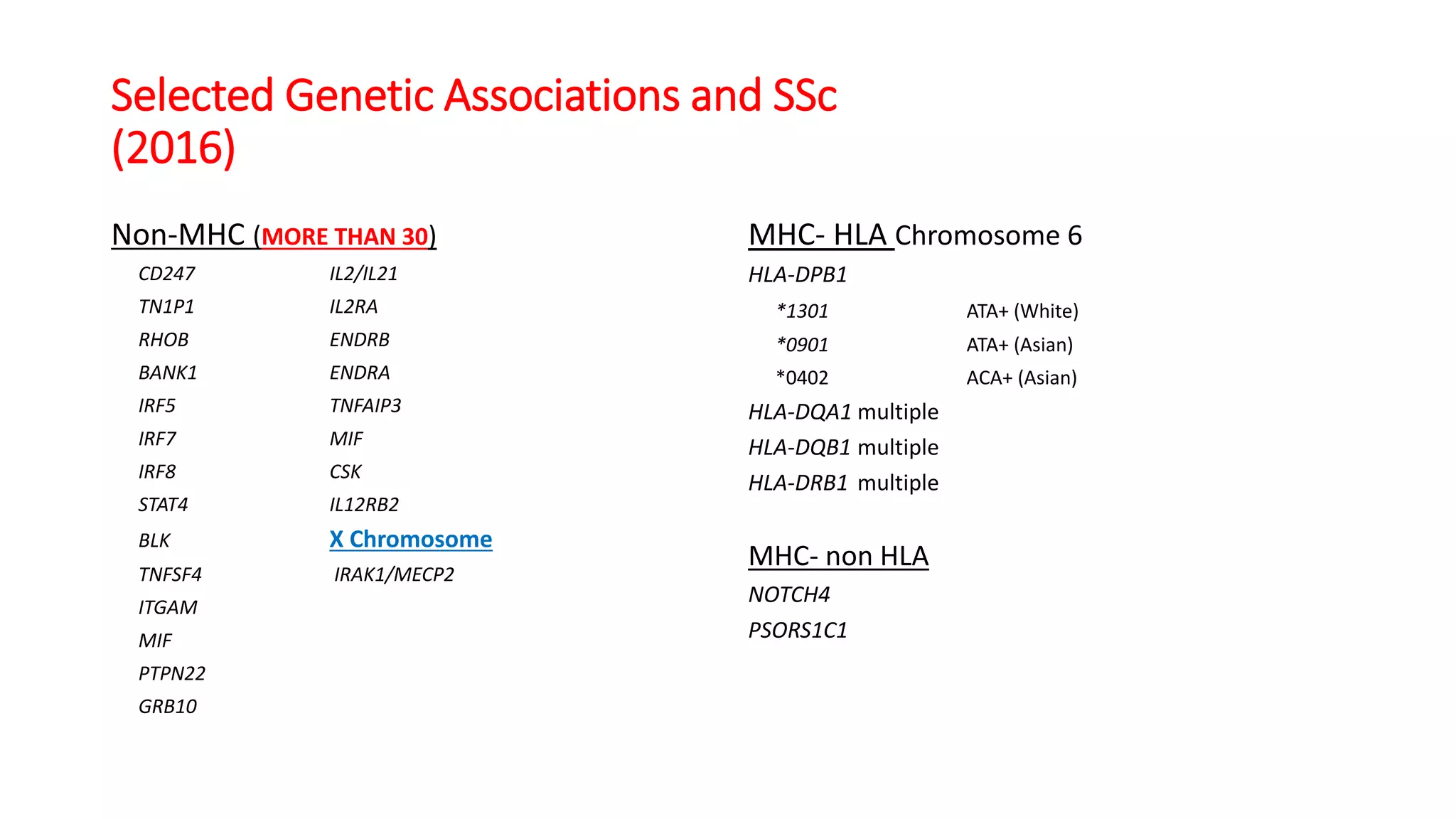
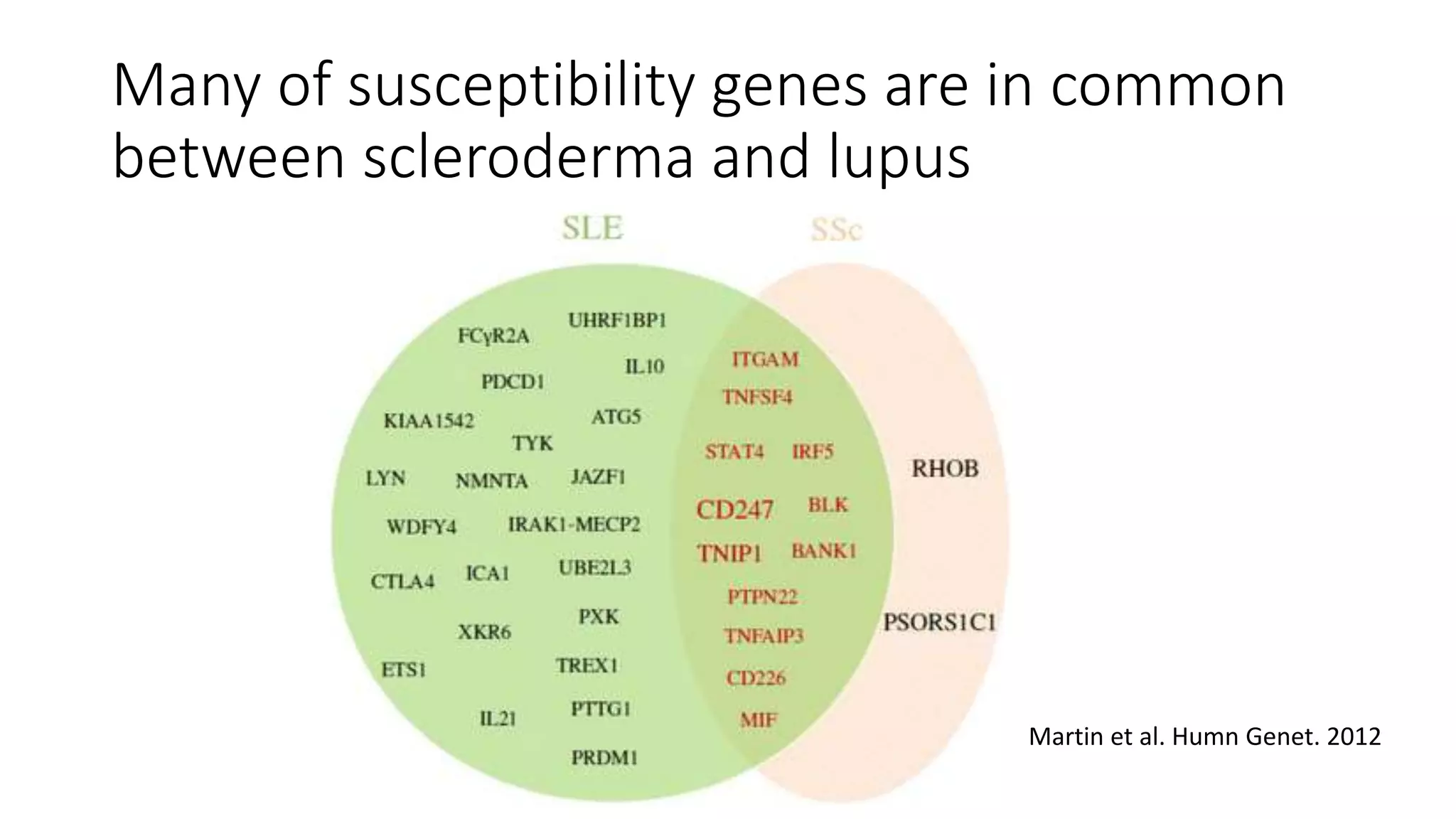
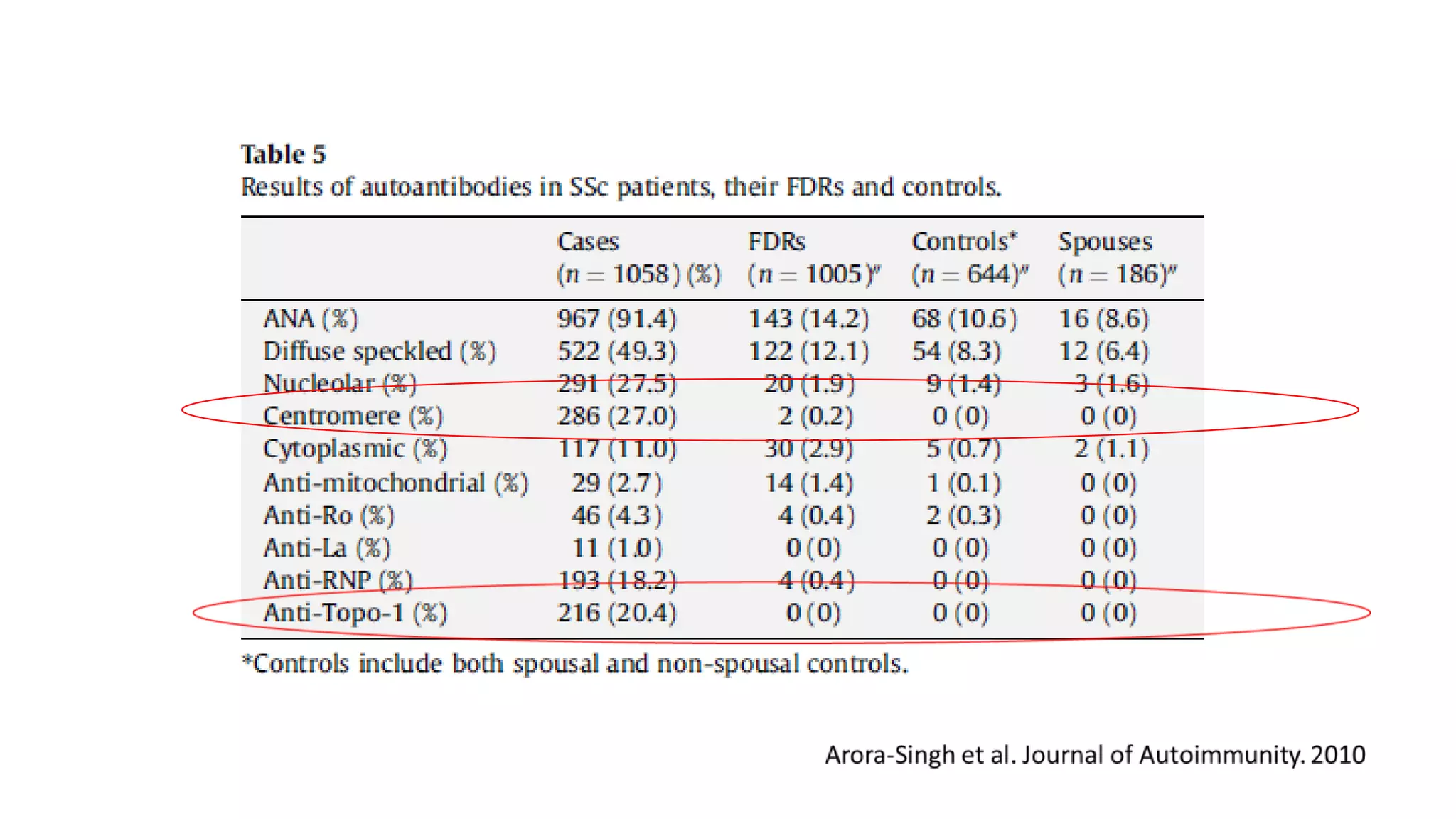
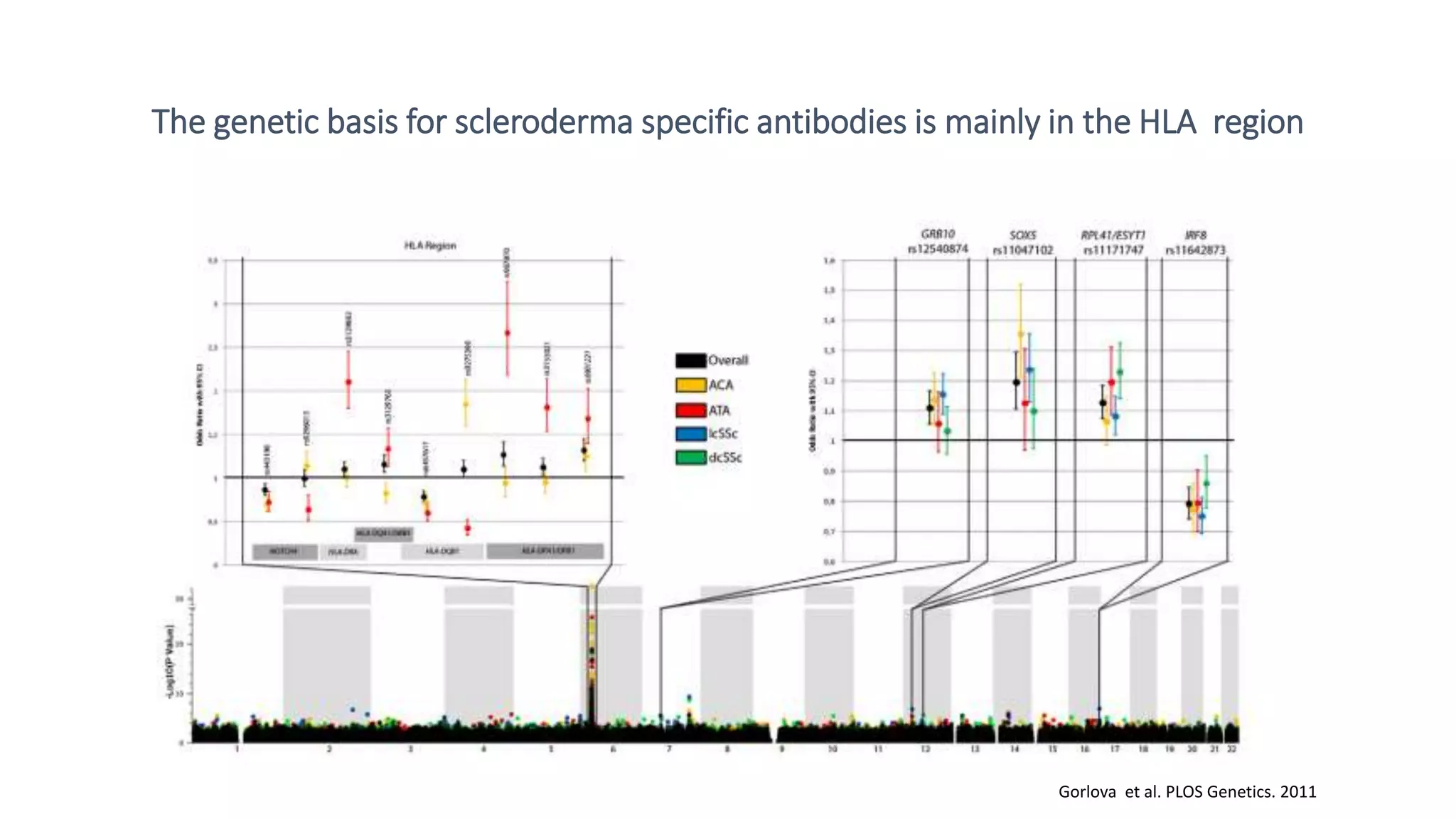


Scleroderma is a complex, polygenic disease influenced by both genetic and environmental factors, with evidence of heritability demonstrated through familial studies. Genetic research, particularly genome-wide association studies (GWAS), has identified over 30 genetic variants associated with scleroderma that primarily affect immune-related pathways. Specific antibodies related to scleroderma exhibit a genetic basis, notably linked to the HLA region on chromosome 6.