Download to read offline



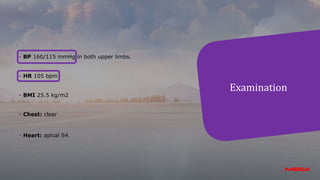
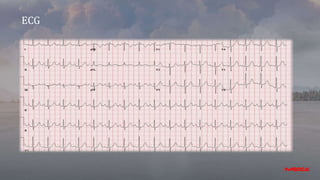












- This document appears to be notes from a case presentation and discussion of treating hypertension. It describes a 50-year-old male patient presenting with shortness of breath, palpitations, and a blood pressure of 160/115 mmHg. Various investigations were conducted. - The discussion centers around hypertension treatment guidelines and determining the appropriate treatment strategy for this patient. Various medication options and their effects are considered. The document recommends starting treatment with a bisoprolol and amlodipine combination to control the patient's blood pressure and heart rate.














![Stress%20 testing housestaff%20didactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101524-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)




























































