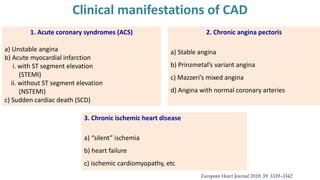
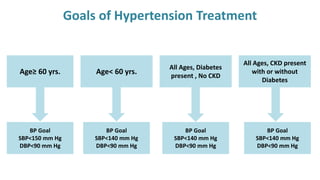
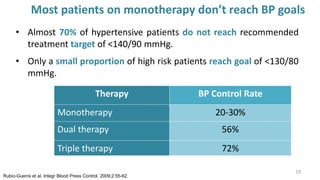
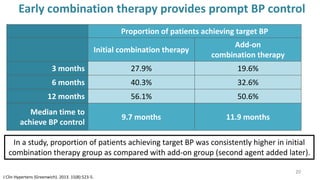
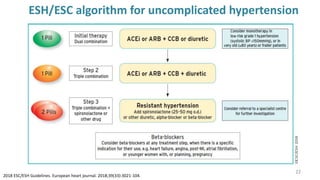
The document discusses hypertension and coronary artery disease (CAD), highlighting the need for tight blood pressure control to prevent cardiovascular complications. It reviews treatment strategies, including lifestyle modifications and the effectiveness of combination therapy with calcium channel blockers and beta-blockers. The findings emphasize that a large proportion of patients do not achieve target blood pressure levels with monotherapy and that combined pharmacotherapy may enhance treatment outcomes.



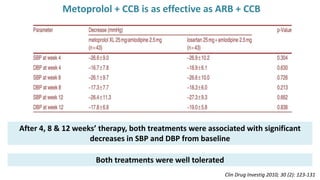
![Metoprolol + CCB effective in the treatment of essential hypertension
Changes in mean blood pressure (BP) throughout the study in responders to metoprolol extended
release 25mg/amlodipine 2.5mg (M/A) [n = 43] or losartan 25mg plus amlodipine 2.5mg (L+A) [n = 43].
DBP= diastolic BP; SBP= systolic BP
Clin Drug Investig 2010; 30 (2): 123-131](https://image.slidesharecdn.com/hypertensioncadmanagementcilacarm-230712182216-16dc69a7/85/HypertensionCAD-Management-Cilacar-M-pptx-44-320.jpg)