This ppt on Routes of drug administration includes introduction, different routes of drug administration, common routes, advantages and disadvantages of different routes and brief explanation on transdermal therapeutic systems.
ROUTES OF DRUGADMINISTRATION
Dr. Anie Jacob
Junior Resident – 1
Department of Pharmacology & Therapeutics
King George’s Medical University, Lucknow
2.
LEARNING OBJECTIVES
1. Todescribe general aspects of different routes of drug
administration.
2. To enumerate the local routes.
3. To enumerate the systemic routes.
4. To understand the importance of different routes of administration.
3.
INTRODUCTION
• Drugs canbe administered by a variety of routes.
• The choice of appropriate route in a given situation depends both on
drug as well as patient related factors.
• Routes can be broadly divided into those for (a) Local action and (b)
Systemic action.
4.
FACTORS GOVERNING CHOICEOF ROUTE
Physical and chemical properties of the drug (solid/liquid/gas;
solubility, pH, irritancy).
Site of desired action- localized and approachable or
generalized and not approachable.
Rate and extent of absorption of the drug from different
routes.
5.
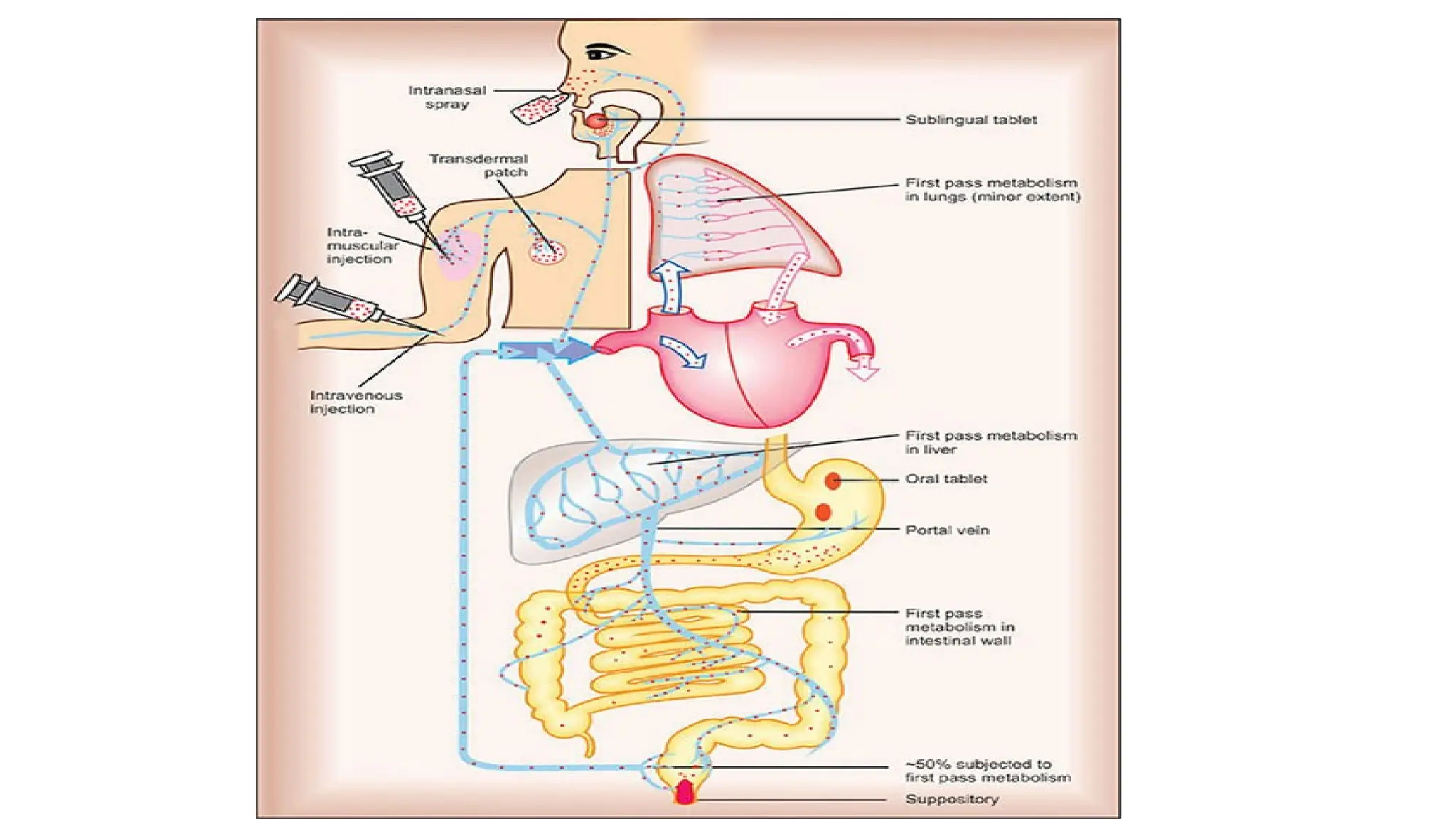
Effect of digestivejuices and first pass metabolism on the drug.
Rapidity with which the response is desired (routine treatment or
emergency).
Condition of the patient (unconscious, vomiting).
6.
LOCAL ROUTES
• Usedfor localized lesions at accessible sites, and for drugs
whose systemic absorption from these sites is minimal or
absent.
• High concentrations are attained at the desired site without
exposing the rest of the body.
• Systemic side effects or toxicity - absent or minimal.
TOPICAL
• External applicationof the drug to the surface for localized action.
• More convenient
• Reassuring to the patient.
9.
• Drugs canbe efficiently delivered to the localized lesions on
skin,
oropharyngeal/ nasal mucosa
Eyes
ear canal,
anal canal or vagina
• in the form of lotion, ointment, cream, powder, rinse, paints, drops,
spray, lozengens, suppositories or pessaries.
10.
DEEPER TISSUES
• Deepareas can be approached by using a syringe and needle, but the
drug should be in such a form that systemic absorption is slow,
• e.g. intra-articular injection (hydrocortisone acetate in knee joint),
• infiltration around a nerve or intrathecal injection (lidocaine),
• retrobulbar injection (hydrocortisone acetate behind the eyeball).
11.
ARTERIAL SUPPLY
• Closeintra-arterial injection - used for contrast media in angiography
• Anticancer drugs can be infused in femoral or brachial artery to
localise the effect for limb malignancies.
12.
SYSTEMIC ROUTES
• Intendedto be absorbed into the blood stream and distributed all over,
including the site of action, through circulation.
• The systemic routes are:
a) Oral
b) Sublingual
c) Rectal
d) Cutaneous
e) Inhalation
f) Nasal
g) Parenteral
14.
ORAL
• Oldest andcommonest
• Safer, more convenient
• Does not need assistance
• Noninvasive, often painless
• Medicament need not be sterile - Cheaper.
• Both solid and liquid dosage forms.
15.
LIMITATIONS OF ORALROUTE
• Action of drugs is slower - not suitable for emergencies.
• Unpalatable drugs (chloramphenicol) are difficult to administer; drug
may be filled in capsules to circumvent this.
• May cause nausea and vomiting.
• Cannot be used for uncooperative/unconscious/ vomiting patient.
• Others are destroyed by digestive juices (penicillin G, insulin)
16.
SUBLINGUAL OR BUCCAL
•The drug is placed under the tongue or crushed in the mouth and
spread over the buccal mucosa.
• Only lipid soluble and non-irritating drugs can be so administered.
• Absorption is relatively rapid- action can be produced in minutes.
• Chief advantage - liver is bypassed
• Drugs given sublingually are-GTN, buprenorphine, desamino-
oxytocin.
17.
RECTAL
• Irritant andunpleasant drugs - suppositories or retention
enema for systemic effect.
• Used – recurrent vomiting / unconscious.
• Inconvenient and embarrassing.
• Absorption is slower, irregular and often unpredictable.
18.
• Diazepam solutionand paracetamol suppository are rapidly and
dependably absorbed from the rectum in children.
• Drug absorbed into external haemorrhoidal veins (about 50%)
bypasses liver, but not that absorbed into internal haemorrhoidal
veins.
• Rectal inflammation can result from irritant drugs.
• Diazepam, indomethacin, paracetamol, ergotamine
19.
CUTANEOUS
• Highly lipidsoluble drugs can be applied over the skin for slow and
prolonged absorption.
• The liver is also bypassed.
• Incorporated in an ointment and applied over specified area of skin.
• Absorption - enhanced by rubbing the preparation, by using an oily
base and by an occlusive dressing.
20.
Transdermal therapeutic systems(TTS)
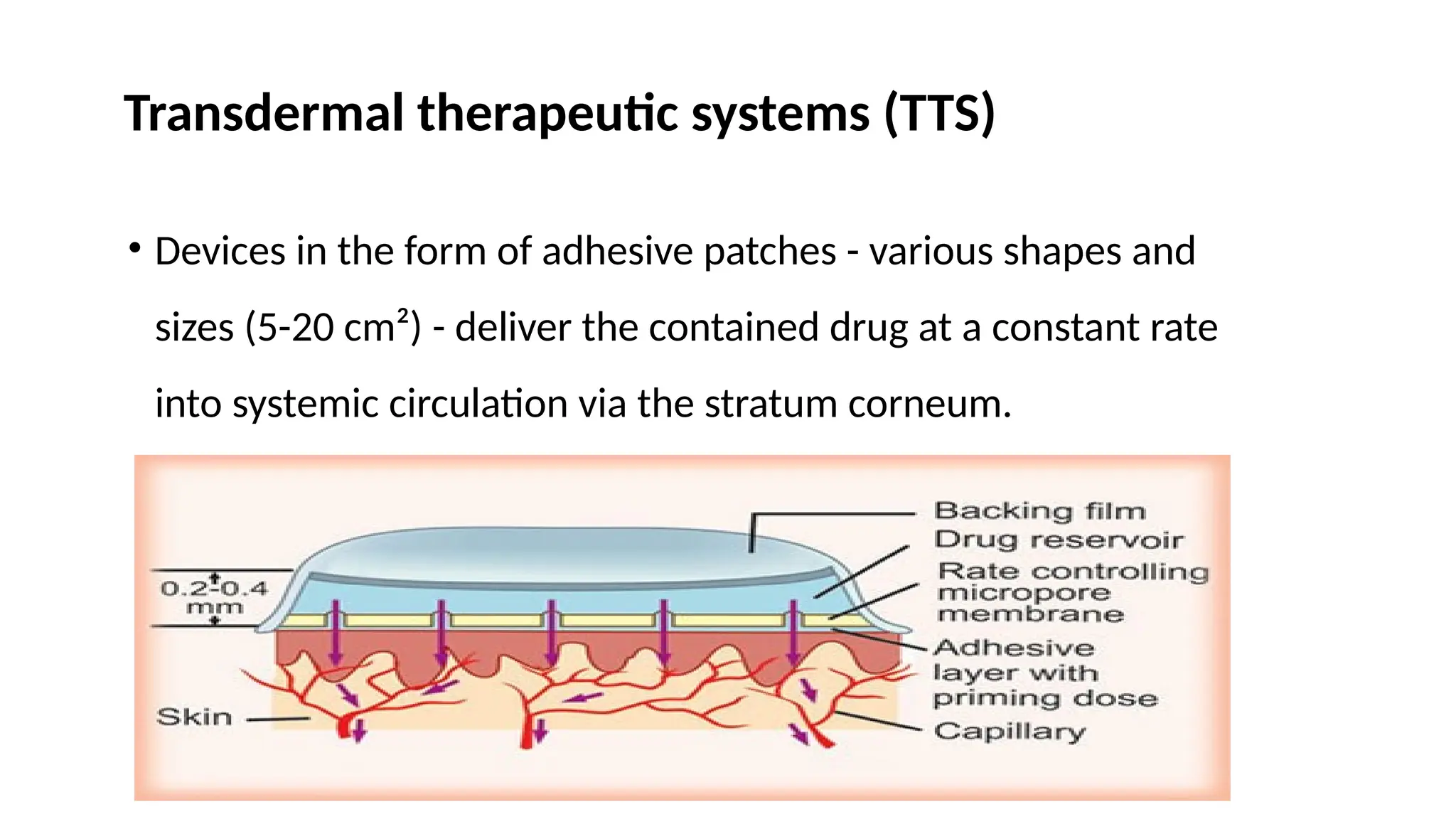
• Devices in the form of adhesive patches - various shapes and
sizes (5-20 cm²) - deliver the contained drug at a constant rate
into systemic circulation via the stratum corneum.
21.
INHALATION
• Volatile liquidsand gases are given by inhalation for systemic action, e.g.
general anaesthetics.
• Absorption takes place from the vast surface of alveoli- action is very rapid.
• Controlled administration is possible with moment to moment adjustment.
• Irritant vapours (ether) cause inflammation of respiratory tract and
increase secretion.
22.
PARENTERAL
• Administration byinjection which takes the drug directly into
the tissue fluid or blood without having to cross the enteral
mucosa.
Advantages:
a) Drug action is faster and surer (Emergencies)
b) Gastric irritation and vomiting are not provoked.
23.
(c) Can beemployed even in unconscious, uncooperative or vomiting
patient.
(d) No chances of interference by food or digestive juices. Liver is bypassed.
Disadvantages:
• The preparation has to be sterilized and is costlier.
• Invasive and painful.
• Assistance of another person is mostly needed
• Chances of local tissue injury.
24.
• The importantparenteral routes are:
a) Subcutaneous (s.c.)
b) Intramuscular (i.m.)
c) Intravenous (i.v.)
d) lntradermal injection
25.
Subcutaneous
• The drugis deposited in the loose subcutaneous tissue which is
richly supplied by nerves.
• Only small volumes can be injected.
• Self-injection is possible.
• Repository (depot) preparations that are aqueous suspensions
can be injected for prolonged action.
• Special forms - Dermojet, Pellet implantation, Sialistic implants.
26.
Intramuscular
• The drugis injected in one of the large skeletal muscles-deltoid,
gluteus maximus, rectus femoris, etc.
• Muscle is less richly supplied with sensory nerves (mild irritants
can be injected) and is more vascular (absorption of drugs in
aqueous solution is faster).
• Less painful, but self injection is often impracticable.
• Avoided - anticoagulant treated patients.
27.
Intravenous
• The drugis injected as a bolus or infused slowly over hours in one of
the superficial veins.
• Drug reaches blood stream directly, effects - produced immediately –
Emergencies.
• The intima of veins is insensitive and drug gets diluted with blood -
highly irritant drugs can be injected i.v.
Intravenous
• Drug dose- required is smallest (bioavailability is I00%) and even
large volumes can be infused.
• Titration of the dose with the response is possible.
• Most risky route- vital organs get exposed to high concentrations of
the drug.
30.
lntradermal injection
• Thedrug is injected into the skin raising a
- bleb
e.g. BCG vaccine, sensitivity testing.
- scarring/multiple puncture of the epidermis through a drop of drug.
• Employed for specific purposes only.
31.
SUMMARY
• The choiceof appropriate route in a given situation depends both on
drug as well as patient related factors.
• Routes can be broadly divided into those for Local action and
Systemic action.
• Local routes – topical, deep tissues, arterial supply
• Systemic routes– Oral, Sublingual, Rectal, Cutaneous, Inhalation,
Nasal, Parenteral.
32.
REFERENCES
• Tripathi KD.Essentials of Medical Pharmacology. 8th ed. New Delhi:
Jaypee Brothers Medical Publishers; 2019. Chapter 1, p. 9-14
• Goodman & Gilman’s. The Pharmacological Basis of Therapeutics.
14th ed. New York: McGraw-Hill; 2023. Chapter 1, p. 26-29