Downloaded 30 times

![© Williams & Wilkins 1998. All Rights Reserved. Published by Lippincott Williams & Wilkins, Inc. 3
Figure 1
Selenium, systemic immune response syndrome, sepsis,
and outcome in critically ill patients.
Forceville, Xavier; Vitoux, Dominique; Gauzit, Remy;
Combes, Alain; Lahilaire, Pierre; Chappuis, Philippe
Critical Care Medicine. 26(9):1536-1544, September
1998.
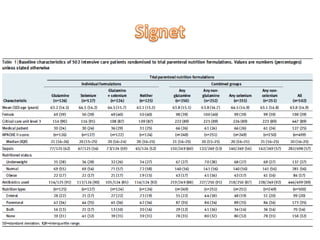
Figure 1 . Admission plasma selenium concentration
related to Acute Physiology and Chronic Health
Evaluation (APACHE) II severity score. Dashed line, mean
+/- SD normal plasma selenium value (1.00 +/- 0.15
[micro sign]mol/L). r2 = .11; p < .0001.](https://image.slidesharecdn.com/1445harris-130515040953-phpapp02/85/Roger-Harris-on-Oxidative-Stress-8-320.jpg)
![© Williams & Wilkins 1998. All Rights Reserved. Published by Lippincott Williams & Wilkins, Inc. 5
Figure 2
Selenium, systemic immune response syndrome, sepsis,
and outcome in critically ill patients.
Forceville, Xavier; Vitoux, Dominique; Gauzit, Remy;
Combes, Alain; Lahilaire, Pierre; Chappuis, Philippe
Critical Care Medicine. 26(9):1536-1544, September
1998.
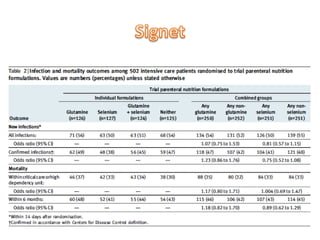
Figure 2 . Admission plasma selenium concentration
related to severity of sepsis. p <or=to .05 for sepsis vs.
severe sepsis; p <or=to .05 for sepsis vs. septic shock
(analysis of variance). Dashed line, mean +/- SD normal
plasma selenium concentration (1.00 +/- 0.15 [micro
sign]mol/L); n, number of patients, including, in
parentheses, number of nonsurviving patients, for each
sepsis severity grade. Values are expressed as median
(middle line in the box) with the top and bottom of the
box encompassing the 25th to the 75th percentiles;
capped lines indicate the tenth to 90th percentiles of the
data; circles, values above the 90th and below the tenth
percentiles.](https://image.slidesharecdn.com/1445harris-130515040953-phpapp02/85/Roger-Harris-on-Oxidative-Stress-9-320.jpg)
![© 1999 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
Figure 1
Selenium replacement in patients with severe systemic
inflammatory response syndrome improves clinical
outcome.
Angstwurm, Matthias; Schottdorf, Juergen; Schopohl,
Jochen; Gaertner, Roland
Critical Care Medicine. 27(9):1807-1813, September
1999.
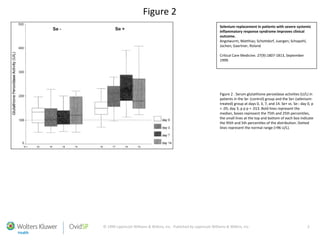
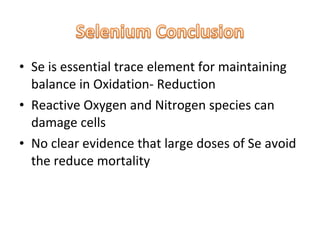
Figure 1 . Serum selenium concentrations ([mu]g/L) in
patients in the Se- (control) group and the Se+ (selenium-
treated) group at days 0, 3, 7, and 14. Se+ vs. Se-: day 0, p
> .05; day 3, p p p = .003. Bold lines represent the
median, boxes represent 75th and 25th percentiles, the
small lines at the top and bottom of each box indicate the
95th and 5th percentiles of the distribution. Dotted lines
represent the normal range (70-120 [mu]g/L, 0.88-1.52
[mu]mol/L).](https://image.slidesharecdn.com/1445harris-130515040953-phpapp02/85/Roger-Harris-on-Oxidative-Stress-12-320.jpg)


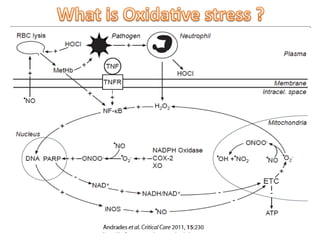
Oxidative stress occurs when there is an imbalance between production of reactive oxygen species and a body's antioxidant defenses. Selenium is an important antioxidant that helps regulate oxidative stress through selenoproteins like glutathione peroxidase. Studies have shown that critically ill patients often have low selenium levels associated with higher illness severity and mortality. Giving selenium supplements to ICU patients increased their selenium and glutathione peroxidase levels and improved clinical outcomes, though larger studies are still needed to determine if selenium reduces mortality.








































































