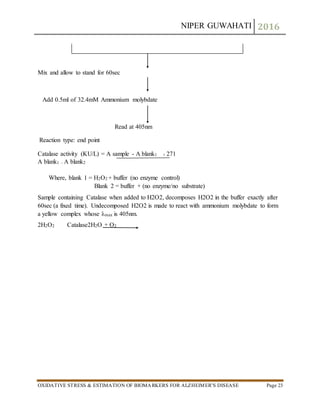
The document discusses oxidative stress and its role in Alzheimer's disease, detailing the nature of free radicals, reactive oxygen species, and antioxidant systems. It highlights how oxidative stress contributes to the pathogenesis of Alzheimer's, leading to neuronal dysfunction and cell death. Furthermore, it outlines various methods for estimating biomarkers related to oxidative stress and antioxidant activity in the context of Alzheimer's research.
![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 2
1.2 TYPES OF FREE RADICALS
Superoxide radical
Hydroxide radical
Nitric oxide radical
Peroxide radicals
H2O2 (non radical).etc
1.3 What are Reactive oxygen species?
Reactive Oxygen Species (ROS) is a phrase used to describe a number of reactive molecules and
free radicals derived from molecular oxygen. The production of oxygen based radicals is the
bane to all aerobic species. These molecules, produced as by-products during the mitochondrial
electron transport of aerobic respiration or by oxidoreductase enzymes and metal catalyzed
oxidation, have the potential to cause a number of deleterious events.
It was originally thought that only phagocytic cells were responsible for ROS production as their
part in host cell defense mechanisms. Recent work has demonstrated that ROS have a role in cell
signaling, including; apoptosis; gene expression; and the activation of cell signalingcascades [1].
ROS are formed as necessary intermediates of metal catalyzed oxidation reactions. Atomic
oxygen has two unpaired electrons in separate orbits in its outer electron shell. This electron](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-2-320.jpg)
![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 3
structure makes oxygen susceptible to radical formation. The sequential reduction of oxygen
through the addition of electrons leads to the formation of a number of ROS including:
superoxide; hydrogen peroxide; hydroxyl radical; hydroxyl ion; and nitric oxide.
1. Superoxide
Superoxide radical (O2¯•) is formed by reduction of oxygen molecule with one electron. In
aqueous solution it is a weak oxidant and acts mainly on ascorbic acid and thiol compounds.
Superoxide radical is a very strong reducing agent and can reduce certain iron complexes, such
as cytochrome C[6]. In vivo, it is decomposed by SOD to hydrogen peroxide and oxygen
2. Hydroxyl radical
Particularly, the most reactive hydroxyl radical, when generated in excess, causes cellular
damage leading to cell death. Hydroxyl radical is generated via the Fenton reaction from
hydrogen peroxide in the presence of ferrous ions or via the Heber- Weiss reaction from
hydrogen peroxide and superoxide radical [2].
3. Nitric oxide
The free radical NO• is synthesized from amino acid L-arginine by vascular endothelial cells,
phagocytes, certain cells in the brain and other cell’s types. Nitric oxide is a vasodilator agent
and possibly an important neurotransmitter. The NO• contains an unpaired electron and is
paramagnetic, it rapidly reacts with O2¯ to form peroxynitrite anion (ONOO¯) in high yield [3].
4. Hydrogen peroxide
Hydrogen peroxide (H2O2) is formed in two ways: indirectly through superoxide anion
dismutation, and directly in some oxidative reactions associated with the transfer of two
electrons to the oxygen. Hydrogen peroxide is a relatively stable in water and appears as a weak
oxidizer and reductant. It is readily diffuses through cell membranes and in the presence of ions
with variable valency it is formed the highly toxic for the cell –hydroxyl radicals [4]. Hydrogen
peroxide is converted by the glutathione peroxidase enzyme to form water and oxygen, thus
preventing the accumulation of precursor to free –radical biosynthesis.
1.4 Whatis oxidative stress?
Oxidative stress is defined as a “state in which oxidation exceeds the antioxidant systems in the
body secondary to a loss of the balance between them.” Disturbance in the balance between the
production of reactive oxygen species (free radicals) and antioxidant defenses.Oxidative stress is
the result of an imbalance in pro-oxidant/antioxidant homeostasis that leads to the generation
of toxic reactive oxygen species [5].oxidative stress has been implicated in the ageing process &
many diseases as shown in below fig.](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-3-320.jpg)

![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 6
2.1Antioxidant defense system(ADS).
A biological antioxidant may be defined as a substance (present in low concentrations compared
to an oxidizable substrate) that significantly delays or inhibits oxidation of a substrate.
Substances that neutralize potential ill effect of free radicals are generally grouped in so called
an Antioxidant defense system (ADS)[6, 7].
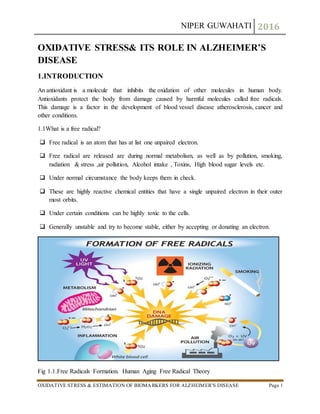
2.2 Mode of Antioxidant defense system(ADS)
Antioxidant defense systems (ADS) traditionally have been termed.
1. Primary defense system 2. Secondary defense system
Primary defense system
Includes antioxidant compounds like a Vitamin A, E, C and Glutathione and uric acid. AO
scavenging enzymes such as peroxidases
Secondary defense system
Includes Lipolytic enzymes, Phospholipases, proteolytic enzymes and DNA repair enzymes
3. THE EFFECTOF OXIDATIVE STRESS:PHYSIOLOGICAL,
ANDBIOCHEMICALMECHANISMS
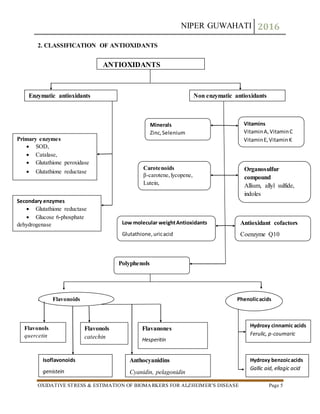
3.1 Effects of Oxidative Stress on DNA
ROS can lead to DNA modifications in several ways, which involves degradation of bases,
single- or double-stranded DNA breaks, purine, pyrimidine or sugar-bound modifications,
mutations, deletions or translocations, and cross-linking with proteins.
Formation of 8-OH-G is the best-known DNA damage occurring via oxidative stress and is
a potential biomarker for carcinogenesis.. Oxidative stress causes instability of microsatellite
(short tandem repeats) regions. Redox active metal ions, hydroxyl radicals increase
microsatellite instability. Even though single-stranded DNA breaks caused by oxidant
injury can easily be tolerated by cells, double-stranded DNA breaks induced by ionizing
radiation can be a significant threat for the cell survival[8].
3.2 Effects of Oxidative Stress on Lipids
ROS can induce lipid peroxidation and disrupt the membrane lipid bilayer arrangement that
may inactivate membrane-bound receptors and enzymes and increase tissue permeability.](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-6-320.jpg)
![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 7
Products of lipid peroxidation, such as MDA and unsaturated aldehydes, are capable of
inactivating many cellular proteins by forming protein cross-linkages. 4-Hydroxy-2-nonenal
causes depletion of intracellular GSH and induces of peroxide production, activates
epidermal growth factor receptor, and induces fibronectin production[9].
Lipid peroxidation products, such as isoprostanes and thiobarbituric acid reactive
substances, have been used as indirect biomarkers of oxidative stress, and increased levels
were shown in thebroncho alveolar lavage fluid or lung of chronic obstructive pulmonary
disease patients or smokers.
3.3 Effects of Oxidative Stress on Proteins
ROS can cause fragmentation of the peptide chain, alteration of electrical charge of proteins,
cross-linking of proteins and oxidation of specific amino acids and therefore lead to
increased susceptibility to proteolysis by degradation by specific proteases.
Cysteine and methionine residues in proteins are particularly more susceptible to oxidation.
Oxidation of sulfhydryl groups or methionine residues of proteins cause conformational
changes, protein unfolding, and degradation.
In some cases, specific oxidation of proteins may take place. For example, methionine can
be oxidized methionine sulfoxide and phenylalanine to o-tyrosine sulfhydryl groups can be
oxidized to form disulfide bonds and carbonyl groups may be introduced into the side chains
of proteins[10].
4. ROLE OF OXIDATIVE STRESS IN ALZHEIMER’S DISEASE
4.1 Alzheimer’s disease
Alzheimer’s disease (AD) is a neurodegenerative disorder associated with a decline in
cognitive impairments, progressive neurodegeneration and formation of amyloid-β (Aβ)
containing plaques and neurofibrillary tangles.
Alzheimer's disease (AD) is a slowly progressive disease of the brain that is characterized by
impairment of memory and eventually by disturbances in reasoning, planning, language, and
perception [11].
Mutations of amyloid precursor protein or presenilin genes or apolipoprotein E gene
polymorphism appear to affect amyloid formation, which in turn causes neuronal death via a](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-7-320.jpg)
![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 8
number of possible mechanisms, including Ca2+ homeostasis disruption, oxidative stress,
excitotoxicity, energy depletion, neuro- inflammation and apoptosis.
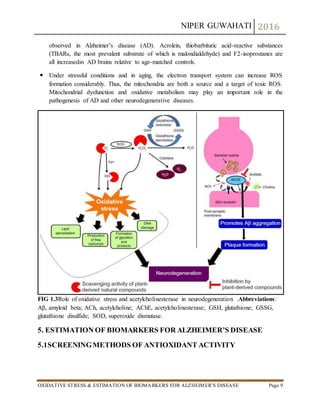
4.2 RELATION OF OXIDATIVE STRESS WITH ALZHEIMER’S DISEASE
Oxidative stress plays a central role in the pathogenesis of AD leading to neuronal
dysfunction and cell death.
Oxidative stress can lead to alterations in cells with an accumulation of oxidized products
such as aldehydes and isoprostanes from lipid peroxidation, protein carbonyls from protein
oxidation, and base adducts from DNA oxidation, all of which serve as markers of
oxidation.
The process of aging is also associated with increased oxidative stress. Through pathological
redox reactions ROS can denature biomolecules such as proteins, lipids and nucleic acids.
This can initiate tissue damage via apoptosis and necrosis[12].
The increased level of oxidative stress in the AD brain is reflected by
increased protein and DNA oxidation,
Decreased level of cytochrome c oxidase and advanced glycosylation end products.
enhanced lipid peroxidation,
Lipid peroxidation can weaken cell membranes causes ion imbalance and impair
metabolism. Oxidative stress can influence DNA methylation which regulates gene
expression. Internalized beta-amyloid may play a role in this process.
Mitochondria are essential for the formation and maintenance of synapses. There is evidence
that oxidative damage precedes pathological changes. Oxidation of mitochondrial DNA
renders it more susceptible to somatic mutation as oxidized bases are frequently misread
during replication. These mutations may initiate erroneous beta-amyloid processing[13].
Beta-amyloid peptide has been shown to inhibit cytochrome oxidase leading to disruption of
the electron transport chain and production of ROS. Thus a viscous cycle may be initiated
that culminates in progressive disease.
Four-hydroxynonenal causes degeneration and death of cultured hippocampal neurons by
impairing ion motive adenosine triphosphatase activity and disrupting calcium homeostasis.
Exposure of cultured hippocampal neurons to amyloid (A) peptide causes a significant
increase in levels of free and protein-bound HNE and increases ROS [14].
4-hydroxy-2,3-nonenal (HNE), acrolein, malondialdehyde (MDA) and F2-isoprostanes are
important break down products of lipid peroxidation. Elevated HNE levels have been](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-8-320.jpg)
![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 10
Various in-vitromethods are used to evaluate the ability of antioxidantto reduce theradical.
Antioxidantactivity can be measured using both serum sample as well as tissue
homogenate[16].
The different in vitro antioxidantscreening methods
Nitric oxide assay
Lipid peroxidation (LPO)
Superoxide Dismustase (SOD)
Reduce Glutathiol (GSH) assay
Glutathione peroxidase (GPx)
Glutathione-s-transferase (GST)
Catalase (CAT)
Glucose 6 phosphatase (G6P)
Creatinine phosphokinase (CPK) etc.
5.2NITRIC OXIDE RADICAL SCAVENGING (NO) ASSAY
Nitric oxide, because of its unpaired electron, is classified as a free radical and displays
important reactivity’s with certain types of proteins and other free radicals.
In vitro inhibition of nitric oxide radical is also a measure of antioxidant activity.
This method is based on the inhibition of nitric oxide radical generated from sodium
nitroprusside in buffer saline and measured by Griess reagent.
In presence of scavengers, the absorbance of the chromophore is evaluated at 546nm.
The activity is expressed as % reduction of nitric oxide.
Procedure
3.0 ml of 10mM sodium nitroprusside in phosphate buffer (pH-7.5) is added to 2.0 ml of
extract and reference compound in different concentrations (20 – 100 µg/ml).
The resulting solutions are then incubated at 25°C for 60 min
A similar procedure is repeated with methanol as blank, which serves as control.](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-10-320.jpg)



![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 14
REAGENTS FOR 2ML FOR 1ML
8.1% SDS 100µl 50µl
0.8% TBA 750µl 375µl
20% Glacial acetic acid 750µl 375µl
Supernatant sample/standard 100µ 50µl
Mix and make up the
volume with distilled water
Make up to 2ml Make up to 1ml
5.4 SUPEROXIDE DISMUTASE (SOD) ASSAY
SOD is a metalloprotein and is the first enzyme involved in theantioxidant defence by
lowering the steady-state level of O2.
Superoxide dismutasesare enzymes that catalyze the dismutation of superoxide into oxygen
and hydrogen peroxide. Thus, they are an important antioxidant defense in nearly all cells
exposed to oxygen[17]. One of the exceedingly rare exceptions is Lactobacillus plantarum
and related lactobacilli, which use a different mechanism
Three forms of superoxide dismutase are present in humans, in all other mammals, and most
chordates. SOD1 is located in the cytoplasm, SOD2 in the mitochondria, and SOD3 is
extracellular. SOD1 and SOD3 contain copper and zinc, whereas SOD2, the mitochondrial
enzyme, has manganese in its reactive centre. The genes are located on chromosomes 21, 6,
and 4, respectively
Mutations in the first SOD enzyme (SOD1) can cause familial amyotrophic lateral sclerosis
(ALS, a form of motor neuron disease) [18].The most common mutation in the U.S. is A4V,
while the most intensely studied isG93A. The other two isoforms of SOD have not been
linked to any human diseases, however, in mice inactivation ofSOD2 causes perinatal
lethality [86] and inactivation of SOD1 causes hepatocellular carcinoma. Mutations inSOD1
can cause familial ALS (several pieces of evidence also show that wild-type SOD1, under
conditions ofcellular stress, is implicated in a significant fraction of sporadic ALS cases,
which represent 90% of ALSpatients [19] by a mechanism that is presently not understood,
but not due to loss of enzymatic activity or a decrease in the conformational stability of the
SOD1 protein. Over expression of SOD1 has been linked to the neural disorders seen in
Down syndrome.
Incubate for 45-60 minutes in
950C in water bath
Cool the system Pink colour will develop
Centrifuge at 10000 g for
10min
Micro titer plate
Absorbance at 530nm
Calculation by standard curve
method](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-14-320.jpg)

![NIPER GUWAHATI 2016
OXIDATIVE STRESS & ESTIMATION OF BIOMARKERS FOR ALZHEIMER’S DISEASE Page 16
After completion of the total reaction, solutions were measured at 412 nm against blank.
Absorbance values were compared with a standard curve generated from standard curve
from known GSH[20, 21].
Preparation of homogenate:
Reagents preparation:
1. GSH Standard Preparation
+
20mM
+
400µM
6.14 mg GSH 1 ml of phosphate buffer (pH7.4)
Solution A
40 µl of solution A 1960µl of phosphate buffer (pH7.4)
Solution B
Use for standard preparation for
GSH](https://image.slidesharecdn.com/oxidativestress-161205012526/85/Oxidative-stress-16-320.jpg)