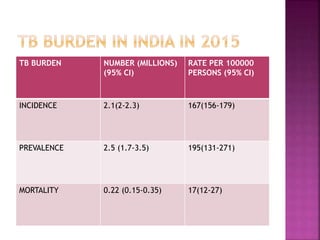
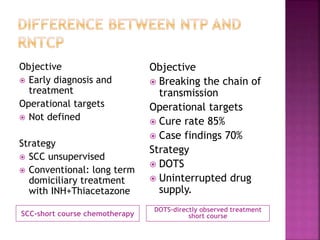
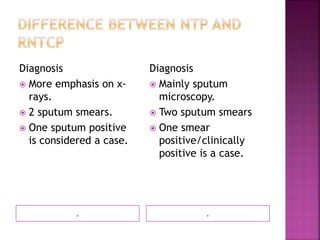
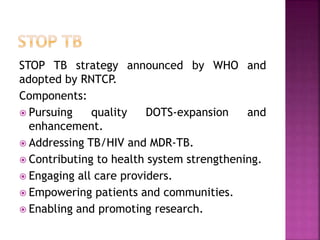
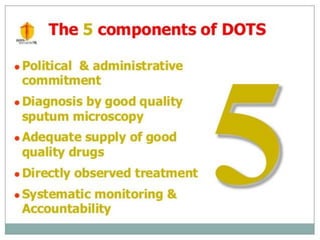
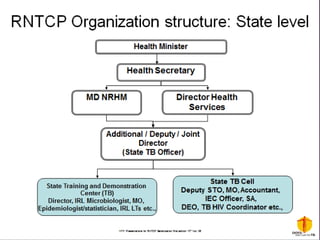
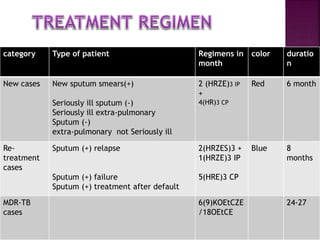
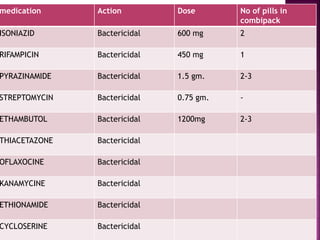
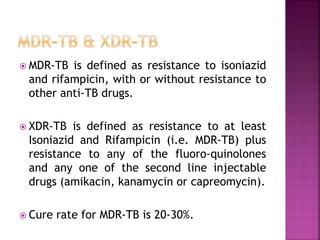
Tuberculosis is one of the top 10 causes of death worldwide, with 10.4 million new cases and 1.7 million deaths in 2016. India has the highest TB burden globally, accounting for over one-fifth of new cases. The document discusses the history and strategies of India's National Tuberculosis Control Programme and Revised National Tuberculosis Control Programme, including the introduction of DOTS strategy. It provides data on TB incidence, prevalence, and mortality in India as well as information on diagnosis, treatment regimens, drug-resistant TB, and the National Strategic Plan 2017-2025's goals to eliminate TB in India.















































![National tuberculosis elimination programme [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nationaltuberculosiseliminationprogrammeautosaved-230623014946-4d00da70-thumbnail.jpg?width=640&height=640&fit=bounds)