The document discusses respiratory physiology and the respiratory system. It covers several key concepts:
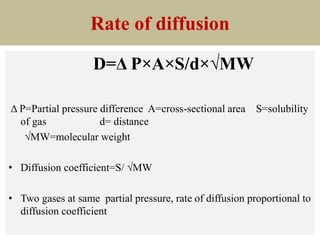
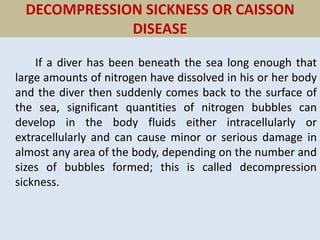
1. It describes Dalton's Law of Partial Pressures and how total gas pressure equals the sum of partial pressures of individual gases.
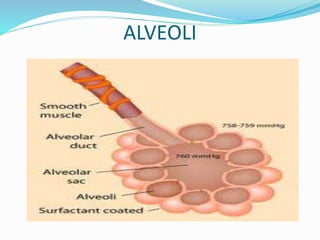
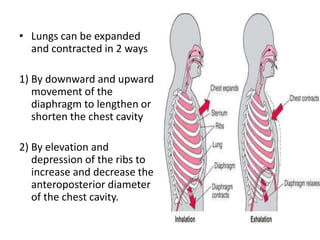
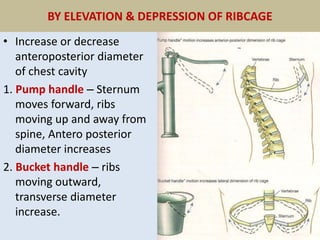
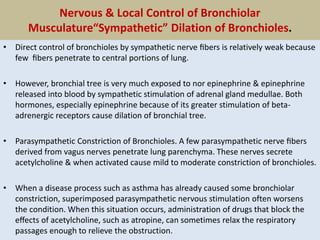
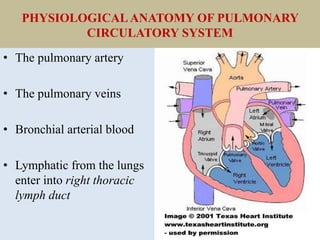
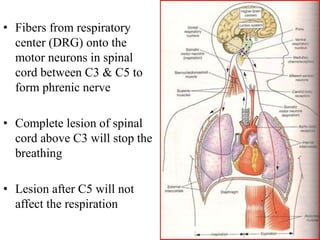
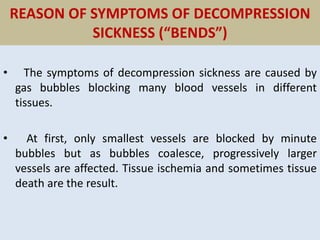
2. It explains the mechanics of breathing including the roles of the diaphragm and rib cage. Inspiration is an active process requiring work.
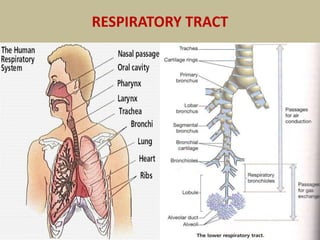
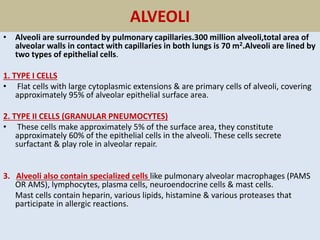
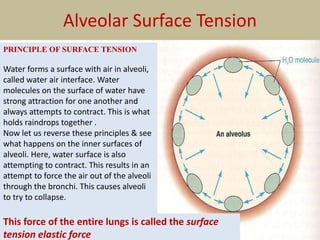
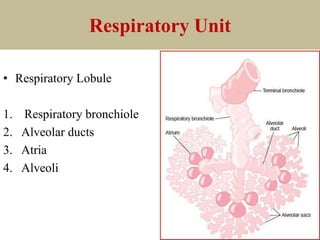
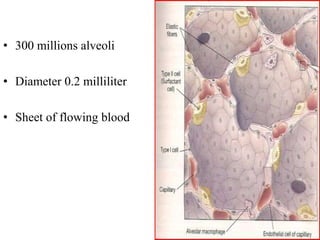
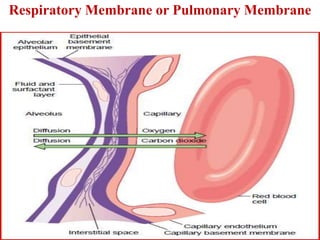
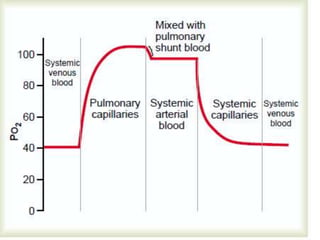
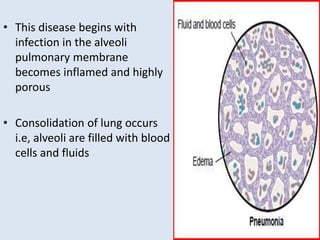
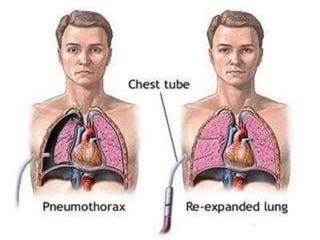
3. It discusses the lungs and alveoli where gas exchange occurs between the blood in pulmonary capillaries and air in alveoli. Surfactant reduces surface tension in the alveoli to prevent their collapse.
4. Several gas laws related to respiration are also covered such as Boyle's Law, Charles' Law,
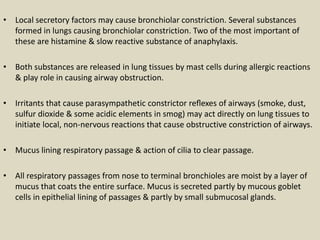
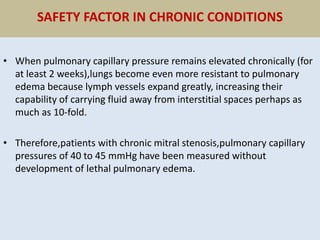
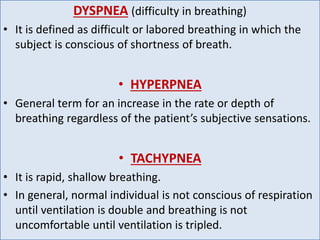
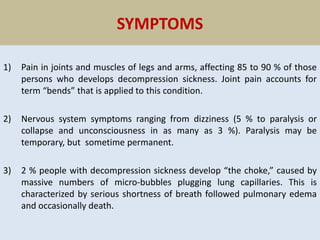
![2. Non respiratory functions /endocrine function
a) Formation of surfactant.
b) Capillary endothelium of respiratory system secretes[ACE] which converts
angiotensin I to angiotensin II that plays role in long term regulation of
blood pressure.
c) Respiratory system plays a role in immune function by
i. Secreting immunoglobulin A (IgA).
ii. Exhibiting phagocytic activity due to presence of macrophages
in alveoli, these are known as pulmonary alveolar macrophages.
d) Respiratory system plays a role in allergic reactions because mast cells are
abundant in respiratory tract. Mast cells play role in allergic reactions by
releasing histamine, bradykinin, prostaglandins and serotonin.](https://image.slidesharecdn.com/respirationbydr-220103090411/85/Respiration-by-dr-mudassar-15-320.jpg)








































![REGULATION OF RESPIRATION lecture note 200L [Autosaved]-1-1.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/regulationofrespirationlecturenote200lautosaved-1-1-250821211712-2266a37b-thumbnail.jpg?width=640&height=640&fit=bounds)
















![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













