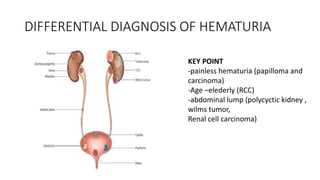
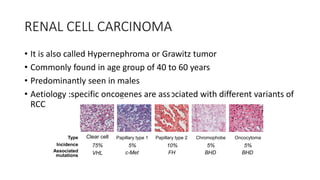
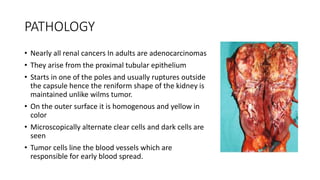
A 60-year-old male presented with painless hematuria and an abdominal lump. On examination, a palpable lump was found. Differential diagnoses included renal cell carcinoma (RCC), given the patient's age and presenting symptoms of hematuria and abdominal lump. RCC is the most common type of kidney cancer in adults. It typically presents in individuals aged 40-60 years and is more common in males. Risk factors include smoking and occupational exposures like asbestos. On pathology, RCC appears as a homogenous yellow mass replacing the renal parenchyma, with microscopically visible clear and dark cells lining blood vessels - explaining its early metastatic potential.
































![Malignant hyperthermia [final]](https://cdn.slidesharecdn.com/ss_thumbnails/malignanthyperthermiafinal-160608094814-thumbnail.jpg?width=640&height=640&fit=bounds)























































