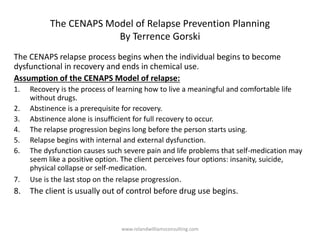
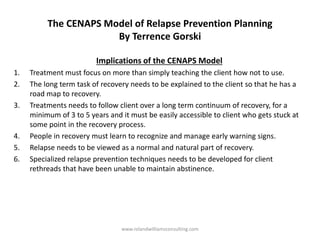
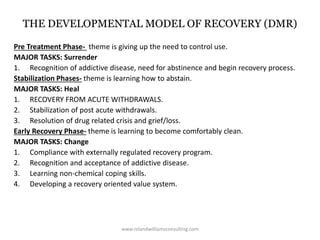
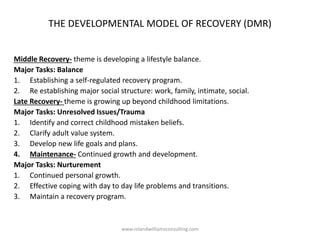
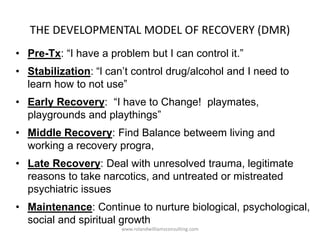
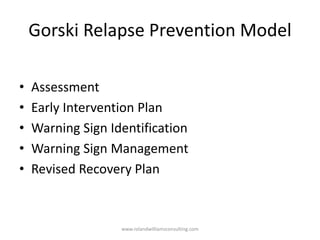
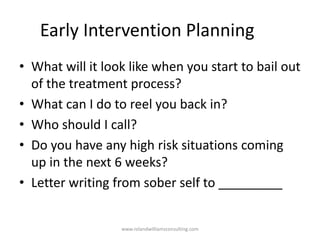
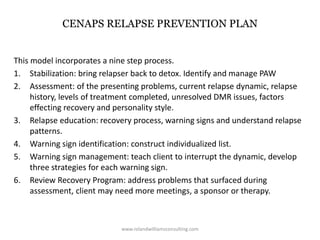
The document discusses relapse prevention counseling strategies for clients with substance use disorders (SUD) and highlights the importance of understanding relapse as a process rather than an event. It outlines various treatment approaches, factors contributing to relapse, the roles of counselors, and effective techniques for relapse prevention. Additionally, it introduces the CENAPS model for relapse prevention, emphasizing the need for long-term support and the management of personal and environmental challenges in recovery.