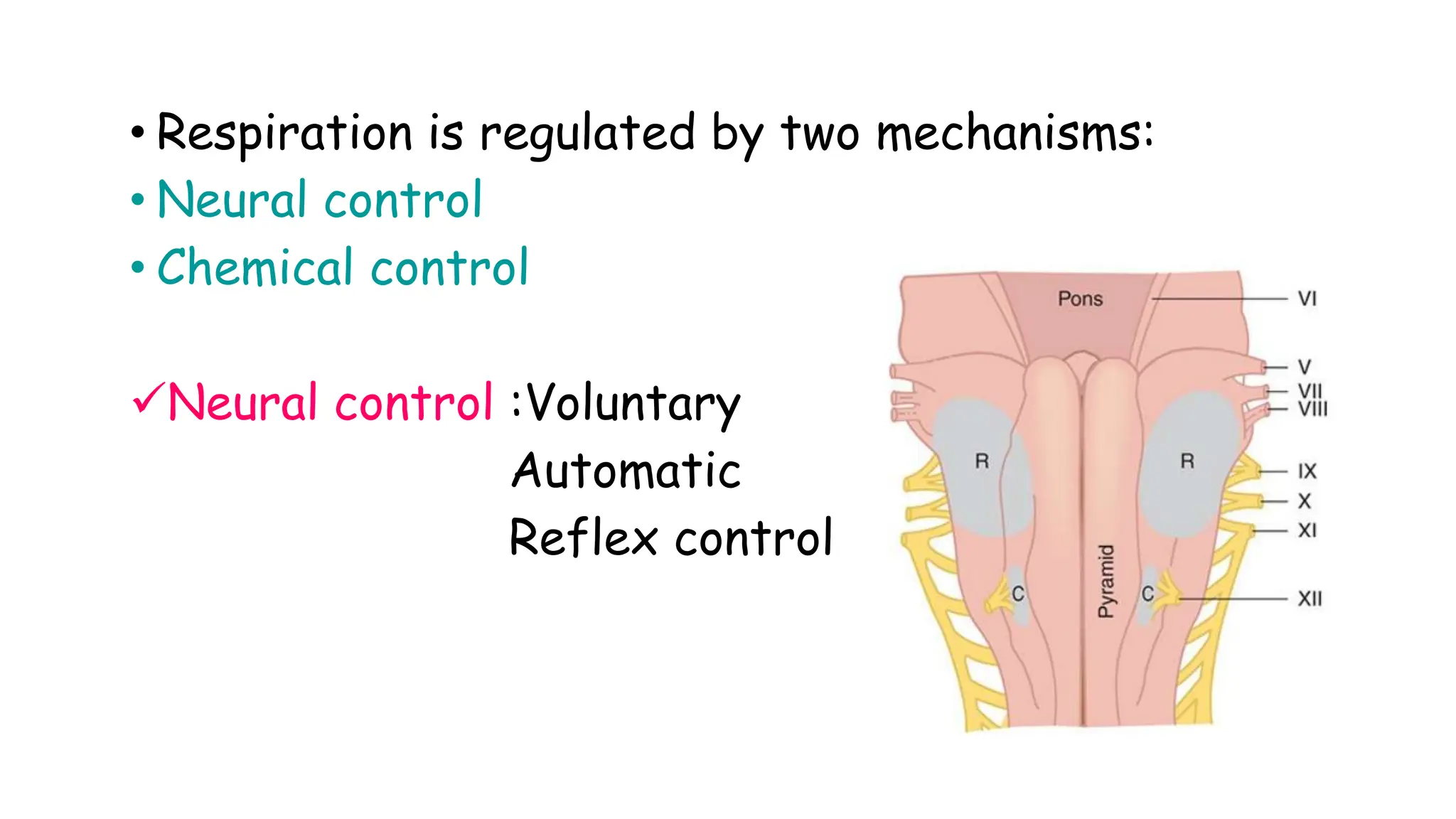
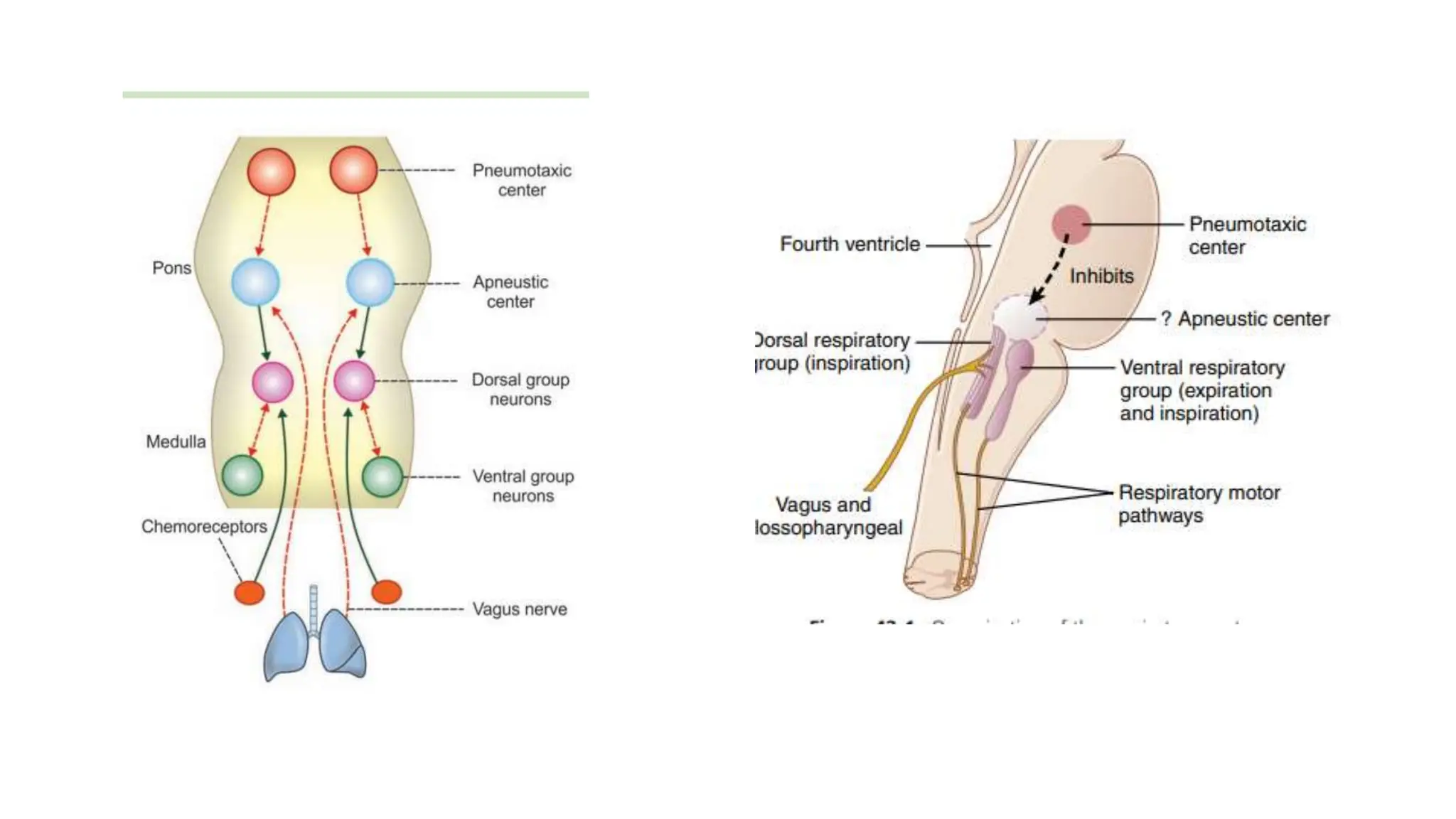
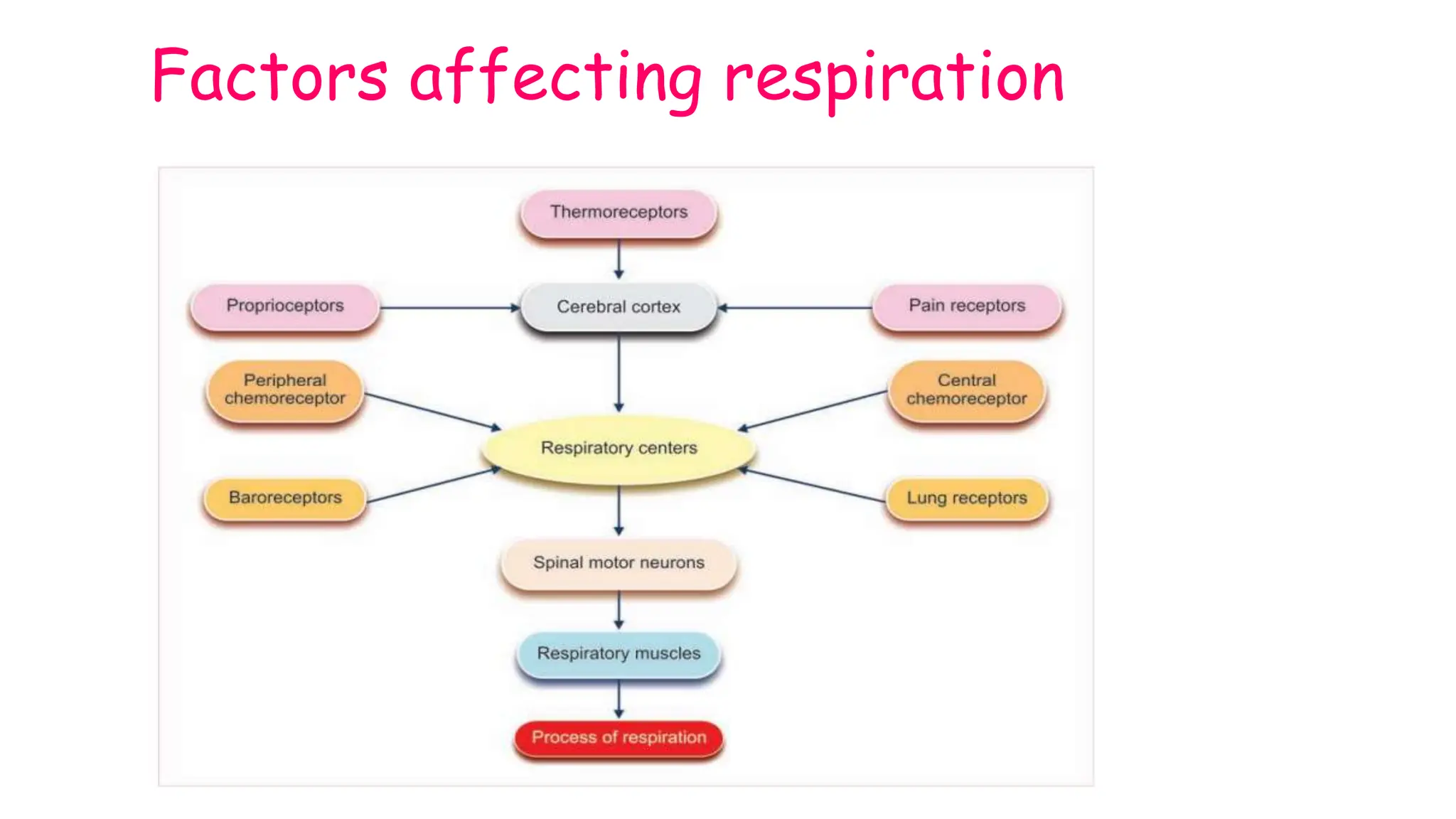
The document details the regulation of respiration, highlighting the neural and chemical controls involved in maintaining arterial blood gas levels. It explains the mechanisms of voluntary and automatic control of breathing, the roles of various respiratory centers in the medulla and pons, and the reflex actions that influence respiratory patterns. Additionally, it discusses the effects of different receptors on respiration and the impact of chemical changes in blood on respiratory regulation.